
Deep Venous Thrombosis and Pulmonary Thromboembolism: Introduction
Epidemiology
Venous thromboembolism (VTE), which encompasses deep venous thrombosis (DVT) and pulmonary embolism (PE), is one of the three major cardiovascular causes of death, along with myocardial infarction and stroke. VTE can cause death from PE or, among survivors, chronic thromboembolic pulmonary hypertension and postphlebitic syndrome. The U.S. Surgeon General has declared that PE is the most common preventable cause of death among hospitalized patients. Medicare has labeled PE and DVT occurring after total hip or knee replacement as unacceptable “never events” and no longer reimburses hospitals for the incremental expenses associated with treating this postoperative complication. New nonprofit organizations have begun educating health care professionals and the public on the medical consequences of VTE, along with risk factors and warning signs.
Between 100,000 and 300,000 VTE-related deaths occur annually in the United States. Mortality rates and length of hospital stay are decreasing as charges for hospital care increase. Approximately three of four symptomatic VTE events occur in the community, and the remainder are hospital acquired. Approximately 14 million (M) hospitalized patients are at moderate to high risk for VTE in the United States annually: 6 M major surgery patients and 8 M medical patients with comorbidities such as heart failure, cancer, and stroke. The prophylaxis paradigm has changed from voluntary to mandatory compliance with guidelines to prevent VTE among hospitalized patients. With an estimated 370,000 PE-related deaths annually in Europe, the projected direct cost for VTE-associated care exceeds 3 billion euros per year. In Japan, as the lifestyle becomes more westernized, the rate of VTE appears to be increasing.
The long-term effects of nonfatal VTE lower the quality of life. Chronic thromboembolic pulmonary hypertension is often disabling and causes breathlessness. A late effect of DVT is postphlebitic syndrome, which eventually occurs in more than one-half of DVT patients. Postphlebitic syndrome (also known as postthrombotic syndrome or chronic venous insufficiency) is a delayed complication of DVT that causes the venous valves of the leg to become incompetent and exude interstitial fluid. Patients complain of chronic ankle or calf swelling and leg aching, especially after prolonged standing. In its most severe form, postphlebitic syndrome causes skin ulceration, especially in the medial malleolus of the leg. There is no effective medical therapy for this condition.
Prothrombotic States
Thrombophilia contributes to the risk of venous thrombosis. The two most common autosomal dominant genetic mutations are factor V Leiden, which causes resistance to activated protein C (which inactivates clotting factors V and VIII), and the prothrombin gene mutation, which increases the plasma prothrombin concentration. Antithrombin, protein C, and protein S are naturally occurring coagulation inhibitors. Deficiencies of these inhibitors are associated with VTE but are rare. Hyperhomocysteinemia can increase the risk of VTE, but lowering the homocysteine level with folate, vitamin B6, or vitamin B12 does not reduce the incidence of VTE. Antiphospholipid antibody syndrome is the most common acquired cause of thrombophilia and is associated with venous or arterial thrombosis. Other common predisposing factors include cancer, systemic arterial hypertension, chronic obstructive pulmonary disease, long-haul air travel, air pollution, obesity, cigarette smoking, eating large amounts of red meat, oral contraceptives, pregnancy, postmenopausal hormone replacement, surgery, and trauma.
Pathophysiology
Embolization
When venous thrombi are dislodged from their site of formation, they embolize to the pulmonary arterial circulation or, paradoxically, to the arterial circulation through a patent foramen ovale or atrial septal defect. About one-half of patients with pelvic vein thrombosis or proximal leg DVT develop PE, which is often asymptomatic. Isolated calf vein thrombi pose a much lower risk of PE but are the most common source of paradoxical embolism. These tiny thrombi can traverse a patent foramen ovale or atrial septal defect, unlike larger, more proximal leg thrombi. With increased use of chronic indwelling central venous catheters for hyperalimentation and chemotherapy, as well as more frequent insertion of permanent pacemakers and internal cardiac defibrillators, upper extremity venous thrombosis is becoming a more common problem. These thrombi rarely embolize and cause PE.
Physiology
The most common gas exchange abnormalities are hypoxemia (decreased arterial PO2) and an increased alveolar-arterial O2 tension gradient, which represents the inefficiency of O2 transfer across the lungs. Anatomic dead space increases because breathed gas does not enter gas exchange units of the lung. Physiologic dead space increases because ventilation to gas exchange units exceeds venous blood flow through the pulmonary capillaries.
Other pathophysiologic abnormalities include the following:
- Increased pulmonary vascular resistance due to vascular obstruction or platelet secretion of vasoconstricting neurohumoral agents such as serotonin. Release of vasoactive mediators can produce ventilation-perfusion mismatching at sites remote from the embolus, thereby accounting for a potential discordance between a small PE and a large alveolar-arterial O2 gradient.
- Impaired gas exchange due to increased alveolar dead space from vascular obstruction, hypoxemia from alveolar hypoventilation relative to perfusion in the nonobstructed lung, right-to-left shunting, and impaired carbon monoxide transfer due to loss of gas exchange surface.
- Alveolar hyperventilation due to reflex stimulation of irritant receptors.
- Increased airway resistance due to constriction of airways distal to the bronchi.
- Decreased pulmonary compliance due to lung edema, lung hemorrhage, or loss of surfactant.
Right-Ventricular (Rv) Dysfunction
Progressive right heart failure is the usual cause of death from PE. As pulmonary vascular resistance increases, RV wall tension rises and causes further RV dilation and dysfunction. RV contraction continues even after the left ventricle (LV) starts relaxing at end-systole. Consequently, the interventricular septum bulges into and compresses an intrinsically normal left ventricle. Diastolic LV impairment develops, attributable to septal displacement, and results in reduced LV distensibility and impaired LV filling during diastole. Increased RV wall tension also compresses the right coronary artery, diminishes subendocardial perfusion, limits myocardial oxygen supply, and may precipitate myocardial ischemia and RV infarction. Underfilling of the LV may lead to a fall in left-ventricular cardiac output and systemic arterial pressure, thereby provoking myocardial ischemia due to compromised coronary artery perfusion. Eventually, circulatory collapse and death may ensue.
Diagnosis
Clinical Evaluation
VTE mimics other illnesses, and PE is known as “the Great Masquerader,” making diagnosis difficult. Occult PE is especially hard to detect when it occurs concomitantly with overt heart failure or pneumonia. In such circumstances, clinical improvement often fails to occur despite standard medical treatment of the concomitant illness. This scenario is a clinical clue to the possible coexistence of PE.
For patients who have DVT, the most common history is a cramp in the lower calf that persists for several days and becomes more uncomfortable as time progresses. For patients who have PE, the most common history is unexplained breathlessness.
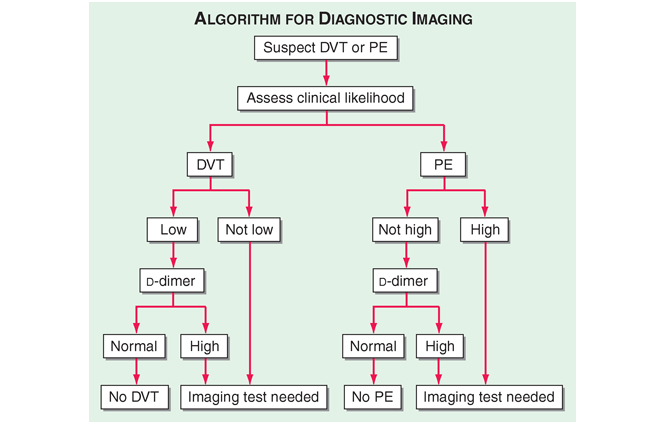
In evaluating patients with possible VTE, the initial task is to decide on the clinical likelihood of the disorder. Patients with a low likelihood of DVT or a low-to-moderate likelihood of PE can undergo initial diagnostic evaluation with d-dimer testing alone (see “Blood tests”) without obligatory imaging tests (Fig. L-1). If the d-dimer is abnormally elevated, imaging tests are the next step.
Point score methods are useful for estimating the clinical likelihood of DVT and PE (Table L-1).
Table L-1 Clinical Decision Rules
Low Clinical Likelihood of DVT if Point Score Is Zero or Less; Moderate-Likelihood Score Is 1 to 2; High-Likelihood Score Is 3 or Greater
| Clinical Variable | Score |
| Active cancer | 1 |
| Paralysis, paresis, or recent cast | 1 |
| Bedridden for >3 days; major surgery <12 weeks | 1 |
| Tenderness along distribution of deep veins | 1 |
| Entire leg swelling | 1 |
| Unilateral calf swelling >3 cm | 1 |
| Pitting edema | 1 |
| Collateral superficial nonvaricose veins | 1 |
| Alternative diagnosis at least as likely as DVT | -2 |
| Clinical Variable | Score |
| Signs and symptoms of DVT | 3.0 |
| Alternative diagnosis less likely than PE | 3.0 |
| Heart rate >100/min | 1.5 |
| Immobilization >3 days; surgery within 4 weeks | 1.5 |
| Prior PE or DVT | 1.5 |
| Hemoptysis | 1.0 |
| Cancer | 1.0 |
Clinical Syndromes
The differential diagnosis is critical because not all leg pain is due to DVT and not all dyspnea is due to PE (Table L-2). Sudden, severe calf discomfort suggests a ruptured Baker’s cyst. Fever and chills usually herald cellulitis rather than DVT, though DVT may be present concomitantly. Physical findings, if present at all, may consist only of mild palpation discomfort in the lower calf. Massive DVT is much easier to recognize. The patient presents with marked thigh swelling and tenderness during palpation of the common femoral vein. In extreme cases, patients are unable to walk or may require a cane, crutches, or a walker.
Table L-2 Differential Diagnosis
| DVT Ruptured Baker’s cyst Cellulitis Postphlebitic syndrome/venous insufficiency |
| PE Pneumonia, asthma, chronic obstructive pulmonary disease Congestive heart failure Pericarditis Pleurisy: “viral syndrome,” costochondritis, musculoskeletal discomfort Rib fracture, pneumothorax Acute coronary syndrome Anxiety |
If the leg is diffusely edematous, DVT is unlikely. More probable is an acute exacerbation of venous insufficiency due to postphlebitic syndrome. Upper extremity venous thrombosis may present with asymmetry in the supraclavicular fossa or in the circumference of the upper arms. A prominent superficial venous pattern may be evident on the anterior chest wall.
Patients with massive PE present with systemic arterial hypotension and usually have anatomically widespread thromboembolism. Those with moderate to large PE have RV hypokinesis on echocardiography but normal systemic arterial pressure. Patients with small to moderate PE have both normal right heart function and normal systemic arterial pressure. They have an excellent prognosis with adequate anticoagulation.
The presence of pulmonary infarction usually indicates a small PE but one that is exquisitely painful because it lodges peripherally, near the innervation of pleural nerves. Pleuritic chest pain is more common with small, peripheral emboli. However, larger, more central PEs can occur concomitantly with peripheral pulmonary infarction.
Nonthrombotic PE may be easily overlooked. Possible etiologies include fat embolism after pelvic or long bone fracture, tumor embolism, bone marrow, and air embolism. Cement embolism and bony fragment embolism can occur after total hip or knee replacement. Intravenous drug users may inject themselves with a wide array of substances that can embolize such as hair, talc, and cotton. Amniotic fluid embolism occurs when fetal membranes leak or tear at the placental margin. Pulmonary edema in this syndrome probably is due to alveolar capillary leakage.
Dyspnea is the most common symptom of PE, and tachypnea is the most common sign. Dyspnea, syncope, hypotension, or cyanosis indicates a massive PE, whereas pleuritic pain, cough, or hemoptysis often suggests a small embolism situated distally near the pleura. On physical examination, young and previously healthy individuals may appear anxious but otherwise seem well, even with an anatomically large PE. They may have dyspnea only with moderate exertion. They often lack “classic” signs such as tachycardia, low-grade fever, neck vein distention, and an accentuated pulmonic component of the second heart sound. Sometimes paradoxical bradycardia occurs.
Nonimaging Diagnostic Modalities
Nonimaging tests are best utilized in combination with clinical likelihood assessment of DVT or PE (Fig. L-1).
Blood Tests
The quantitative plasma d-dimer enzyme-linked immunosorbent assay (ELISA) rises in the presence of DVT or PE because of the breakdown of fibrin by plasmin. Elevation of d-dimer indicates endogenous although often clinically ineffective thrombolysis. The sensitivity of the d-dimer is >80% for DVT (including isolated calf DVT) and >95% for PE. The d-dimer is less sensitive for DVT than for PE because the DVT thrombus size is smaller. The d-dimer is a useful “rule out” test. More than 95% of patients with a normal (<500 ng/mL) d-dimer do not have PE. The d-dimer assay is not specific. Levels increase in patients with myocardial infarction, pneumonia, sepsis, cancer, and the postoperative state and those in the second or third trimester of pregnancy. Therefore, d-dimer rarely has a useful role among hospitalized patients, because levels are frequently elevated due to systemic illness.
Contrary to classic teaching, arterial blood gases lack diagnostic utility for PE, even though both PO2 and Pco2 often decrease. Among patients suspected of having PE, neither the room air arterial PO2 nor calculation of the alveolar-arterial O2 gradient can reliably differentiate or triage patients who actually have PE at angiography.
Elevated Cardiac Biomarkers
Serum troponin and plasma heart-type fatty acid–binding protein levels increase because of RV microinfarction. Myocardial stretch results in elevation of brain natriuretic peptide or NT-pro-brain natriuretic peptide. Elevated cardiac biomarkers predict an increase in major complications and mortality from PE.
Electrocardiogram
The most frequently cited abnormality, in addition to sinus tachycardia, is the S1Q3T3 sign: an S wave in lead I, a Q wave in lead III, and an inverted T wave in lead III . This finding is relatively specific but insensitive. Perhaps the most common abnormality is T-wave inversion in leads V1 to V4.
Noninvasive Imaging Modalities
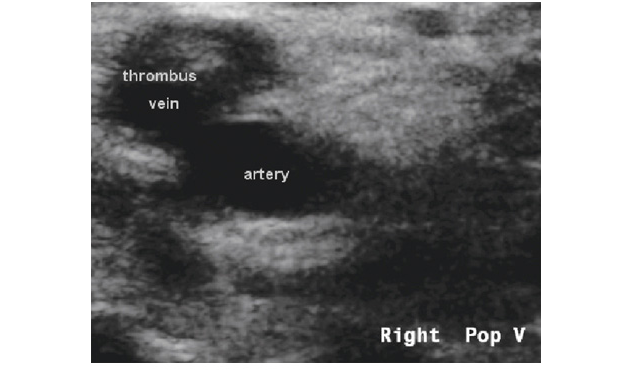
Ultrasonography of the deep venous system (Table L-3) relies on loss of vein compressibility as the primary criterion for DVT. When a normal vein is imaged in cross-section, it readily collapses with gentle manual pressure from the ultrasound transducer. This creates the illusion of a “wink.” With acute DVT, the vein loses its compressibility because of passive distention by acute thrombus. The diagnosis of acute DVT is even more secure when thrombus is directly visualized. It appears homogeneous and has low echogenicity (Fig. L-2). The vein itself often appears mildly dilated, and collateral channels may be absent.
| Table L-3 Ultrasonography of the Deep Leg Veins |
| Criteria for Establishing the Diagnosis of Acute DVT |
| Lack of vein compressibility (principal criterion) Vein does not “wink” when gently compressed in cross-section Failure to appose walls of vein due to passive distention |
| Direct Visualization of Thrombus |
| Homogeneous Low echogenicity |
| Abnormal Doppler Flow Dynamics |
| Normal response: calf compression augments Doppler flow signal and confirms vein patency proximal and distal to Doppler Abnormal response: flow blunted rather than augmented with calf compression |
Venous flow dynamics can be examined with Doppler imaging. Normally, manual calf compression causes augmentation of the Doppler flow pattern. Loss of normal respiratory variation is caused by an obstructing DVT or by any obstructive process within the pelvis. Because DVT and PE are so closely related and are both treated with anticoagulation (see “Treatment Deep Venous Thrombosis”) confirmed DVT is usually an adequate surrogate for PE. In contrast, a normal venous ultrasound does not exclude PE. About one-half of patients with PE have no imaging evidence of DVT, probably because the clot already has embolized to the lung or is in the pelvic veins, where ultrasonography is usually inadequate. In patients without DVT, the ultrasound examination may identify other reasons for leg discomfort, such as a Baker’s cyst (also known as a popliteal or synovial cyst) or a hematoma. For patients with a technically poor or nondiagnostic venous ultrasound, one should consider alternative imaging modalities for DVT, such as computed tomography (CT) and magnetic resonance imaging.
Chest Roentgenography
A normal or nearly normal chest x-ray often occurs in PE. Well-established abnormalities include focal oligemia (Westermark’s sign), a peripheral wedged-shaped density above the diaphragm (Hampton’s hump), and an enlarged right descending pulmonary artery (Palla’s sign).
Chest CT
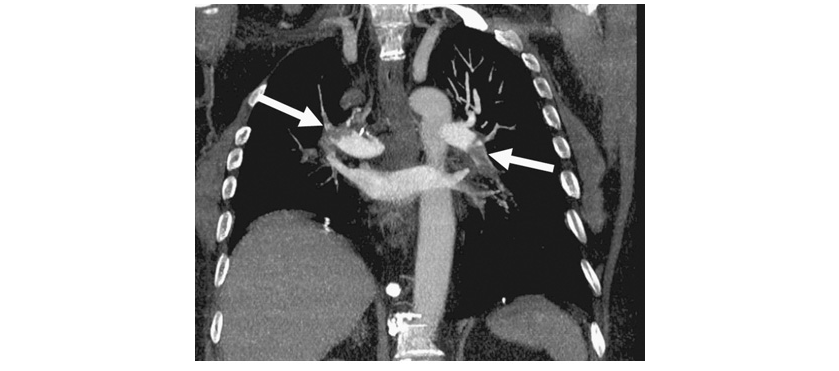
Computed tomography of the chest with intravenous contrast is the principal imaging test for the diagnosis of PE (Fig. L-3). Multidetector-row spiral CT acquires all chest images with ≤1 mm of resolution during a short breath hold. This generation of CT scanners can image small peripheral emboli. Sixth-order branches can be visualized with resolution superior to that of conventional invasive contrast pulmonary angiography. The CT scan also obtains excellent images of the RV and LV and can be used for risk stratification along with its use as a diagnostic tool. In patients with PE, RV enlargement on chest CT indicates an increased likelihood of death within the next 30 days compared with PE patients who have normal RV size on chest CT. When imaging is continued below the chest to the knee, pelvic and proximal leg DVT also can be diagnosed by CT scanning. In patients without PE, the lung parenchymal images may establish alternative diagnoses not apparent on chest x-ray that explain the presenting symptoms and signs such as pneumonia, emphysema, pulmonary fibrosis, pulmonary mass, and aortic pathology. Sometimes asymptomatic early-stage lung cancer is diagnosed incidentally.
Lung Scanning
Lung scanning has become a second-line diagnostic test for PE, used mostly for patients who cannot tolerate intravenous contrast. Small particulate aggregates of albumin labeled with a gamma-emitting radionuclide are injected intravenously and are trapped in the pulmonary capillary bed. The perfusion scan defect indicates absent or decreased blood flow, possibly due to PE. Ventilation scans, obtained with a radiolabeled inhaled gas such as xenon or krypton, improve the specificity of the perfusion scan. Abnormal ventilation scans indicate abnormal nonventilated lung, thereby providing possible explanations for perfusion defects other than acute PE, such as asthma and chronic obstructive pulmonary disease. A high-probability scan for PE is defined as one that indicates two or more segmental perfusion defects in the presence of normal ventilation.
The diagnosis of PE is very unlikely in patients with normal and nearly normal scans but is about 90% certain in patients with high-probability scans. Unfortunately, most patients have nondiagnostic scans, and fewer than one-half of patients with angiographically confirmed PE have a high probability scan. As many as 40% of patients with high clinical suspicion for PE and “low-probability” scans do, in fact, have PE at angiography.
Magnetic Resonance (MR) (Contrast-Enhanced)
When ultrasound is equivocal, MR venography with gadolinium contrast is an excellent imaging modality to diagnose DVT. MR imaging should be considered for suspected VTE patients with renal insufficiency or contrast dye allergy. MR pulmonary angiography may detect large proximal PE but is not reliable for smaller segmental and subsegmental PE.
Echocardiography
Echocardiography is not a reliable diagnostic imaging tool for acute PE because most patients with PE have normal echocardiograms. However, echocardiography is a very useful diagnostic tool for detecting conditions that may mimic PE, such as acute myocardial infarction, pericardial tamponade, and aortic dissection.
Transthoracic echocardiography rarely images thrombus directly. The best-known indirect sign of PE on transthoracic echocardiography is McConnell’s sign: hypokinesis of the RV free wall with normal motion of the RV apex.
One should consider transesophageal echocardiography when CT scanning facilities are not available or when a patient has renal failure or severe contrast allergy that precludes administration of contrast despite premedication with high-dose steroids. This imaging modality can identify saddle, right main, or left main PE.
Invasive Diagnostic Modalities
Pulmonary Angiography
Chest CT with contrast (see above) has virtually replaced invasive pulmonary angiography as a diagnostic test. Invasive catheter-based diagnostic testing is reserved for patients with technically unsatisfactory chest CTs and those in whom an interventional procedure such as catheter-directed thrombolysis or embolectomy is planned. A definitive diagnosis of PE depends on visualization of an intraluminal filling defect in more than one projection. Secondary signs of PE include abrupt occlusion (“cut-off”) of vessels, segmental oligemia or avascularity, a prolonged arterial phase with slow filling, and tortuous, tapering peripheral vessels.
Contrast Phlebography
Venous ultrasonography has virtually replaced contrast phlebography as the diagnostic test for suspected DVT.
Integrated Diagnostic Approach
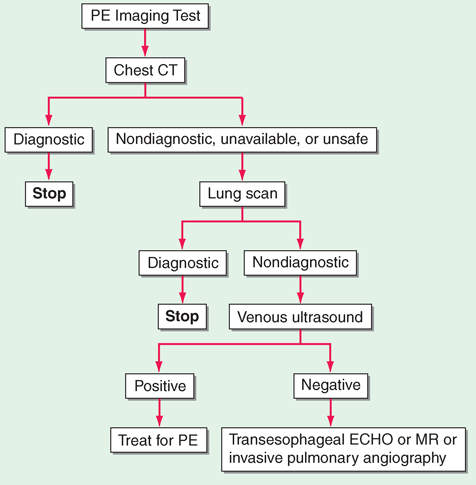
An integrated diagnostic approach (Fig. L-1) streamlines the workup of suspected DVT and PE (Fig. L-4).

Treatment: Deep Venous Thrombosis
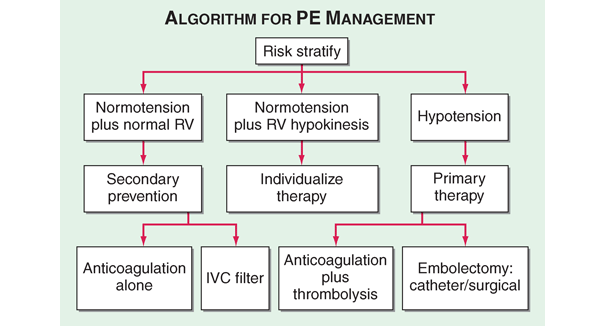
Primary Therapy versus Secondary Prevention
Primary therapy consists of clot dissolution with thrombolysis or removal of PE by embolectomy. Anticoagulation with heparin and warfarin or placement of an inferior vena caval filter constitutes secondary prevention of recurrent PE rather than primary therapy.
Risk Stratification
Rapid and accurate risk stratification is critical in determining the optimal treatment strategy. The presence of hemodynamic instability, RV dysfunction, RV enlargement, or elevation of the troponin level due to RV microinfarction can identify high-risk patients. RV hypokinesis on echocardiography, RV enlargement on chest CT, and troponin elevation predict an increased mortality rate from PE.
Primary therapy should be reserved for patients at high risk of an adverse clinical outcome. When RV function remains normal in a hemodynamically stable patient, a good clinical outcome is highly likely with anticoagulation alone (Fig. L-5).
Treatment: Massive Pulmonary Embolism
Anticoagulation
Anticoagulation is the foundation for successful treatment of DVT and PE (Table L-4). Immediately effective anticoagulation is initiated with a parenteral drug: unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or fondaparinux. One should use a direct thrombin inhibitor—argatroban, lepirudin, or bivalirudin—in patients with proven or suspected heparin-induced thrombocytopenia. Parenteral agents are continued as a transition or “bridge” to stable, long-term anticoagulation with a vitamin K antagonist (exclusively warfarin in the United States). Warfarin requires 5–7 days to achieve a therapeutic effect. During that period, one should overlap the parenteral and oral agents. After 5–7 days of anticoagulation, residual thrombus begins to endothelialize in the vein or pulmonary artery. However, anticoagulants do not directly dissolve thrombus that already exists.
| Table L-4 Anticoagulation of VTE |
| Immediate Parenteral Anticoagulation |
| Unfractionated heparin, bolus and continuous infusion, to achieve aPTT two to three times the upper limit of the laboratory normal, or Enoxaparin 1 mg/kg twice daily with normal renal function, or Dalteparin 200 U/kg once daily or 100 U/kg twice daily, with normal renal function, or Tinzaparin 175 U/kg once daily with normal renal function, or Fondaparinux weight-based once daily; adjust for impaired renal function |
| Warfarin Anticoagulation |
| Usual start dose is 5 mg Titrate to INR, target 2.0–3.0 Continue parenteral anticoagulation for a minimum of 5 days and until two sequential INR values, at least 1 day apart, achieve the target INR range. |
Unfractionated Heparin
Unfractionated heparin anticoagulates by binding to and accelerating the activity of antithrombin, thus preventing additional thrombus formation and permitting endogenous fibrinolytic mechanisms to lyse clot that already has formed. UFH is dosed to achieve a target activated partial thromboplastin time (aPTT) that is 2–3 times the upper limit of the laboratory normal. This is usually equivalent to an aPTT of 60–80 s. For UFH, a typical intravenous bolus is 5000–10,000 units followed by a continuous infusion of 1000–1500 U/h. Nomograms based on a patient’s weight may assist in adjusting the dose of heparin. The most popular nomogram utilizes an initial bolus of 80 U/kg, followed by an initial infusion rate of 18/kg per h.
The major advantage of UFH is its short half-life. This is especially useful if the patient may undergo an invasive procedure such as embolectomy. The major disadvantage of UFH is that achieving the target aPTT is empirical and may require repeated blood sampling and heparin dose adjustment every 4–6 hours. Furthermore, patients are at risk of developing heparin-induced thrombocytopenia.
Low-Molecular-Weight Heparins
These fragments of UFH exhibit less binding to plasma proteins and endothelial cells and consequently have greater bioavailability, a more predictable dose response, and a longer half-life than does UFH. No monitoring or dose adjustment is needed unless the patient is markedly obese or has chronic kidney disease.
There are two commonly used LMWH preparations in the United States: enoxaparin and dalteparin. Enoxaparin is approved as a bridge to warfarin for VTE. Dalteparin is also approved as monotherapy without warfarin for symptomatic VTE patients with cancer in a dose of 200 U/kg once daily for 30 days, followed by 150 U/kg once daily for months 2–6. These weight-adjusted LMWH doses must be reduced in patients with chronic kidney disease because the kidneys metabolize LMWH.
Fondaparinux
Fondaparinux, an anti-Xa pentasaccharide, is administered as a once-daily subcutaneous injection in a prefilled syringe to treat DVT and PE as a “bridge” to warfarin. No laboratory monitoring is required. Patients weighing <50 kg receive 5 mg, patients weighing 50–100 kg receive 7.5 mg, and patients weighing >100 kg receive 10 mg. Fondaparinux is synthesized in a laboratory and, unlike LMWH or UFH, is not derived from animal products. It does not cause heparin-induced thrombocytopenia. The dose must be adjusted downward for patients with renal dysfunction because the kidneys metabolize the drug.
Warfarin
This vitamin K antagonist prevents carboxylation activation of coagulation factors II, VII, IX, and X. The full effect of warfarin requires at least 5 days even if the prothrombin time, used for monitoring, becomes elevated more rapidly. If warfarin is initiated as monotherapy during an acute thrombotic illness, a paradoxical exacerbation of hypercoagulability can increase the likelihood of thrombosis rather than prevent it. Overlapping UFH, LMWH, or fondaparinux with warfarin for at least 5 days can counteract the early procoagulant effect of unopposed warfarin.
Warfarin Dosing
In an average-size adult, warfarin usually is initiated in a dose of 5 mg. Doses of 7.5 or 10 mg can be used in obese or large-framed young patients who are otherwise healthy. Patients who are malnourished or who have received prolonged courses of antibiotics are probably deficient in vitamin K and should receive smaller initial doses of warfarin, such as 2.5 mg. The prothrombin time is standardized by calculating the international normalized ratio (INR), which assesses the anticoagulant effect of warfarin . The target INR is usually 2.5, with a range of 2.0–3.0.
The warfarin dose is titrated to achieve the target INR. Proper dosing is difficult because hundreds of drug-drug and drug-food interactions affect warfarin metabolism. Variables such as increasing age and comorbidities such as systemic illness reduce the required warfarin dose. Pharmacogenomics may provide more precise initial dosing of warfarin, especially for patients who require unusually large or small doses. CYP2C9 variant alleles impair the hydroxylation of S-warfarin, thereby lowering the dose requirement. Variants in the gene encoding the vitamin K epoxide reductase complex 1 (VKORC1) can predict whether patients require low, moderate, or high warfarin doses. Nevertheless, more than half of warfarin dosing variability is caused by clinical factors such as age, sex, weight, concomitant drugs, and comorbid illnesses.
Nomograms have been developed (www.warfarindosing.org) to help clinicians initiate warfarin dosing based on clinical information and, if available, pharmacogenetic data. However, most practitioners utilize empirical dosing with an “educated guess.” Centralized anticoagulation clinics have improved the efficacy and safety of warfarin dosing. Patients maintain a therapeutic INR more often if they self-monitor their INR with a home point-of-care fingerstick machine rather than obtaining a coagulation laboratory INR. The patient subgroup with the best results self-adjusts warfarin doses as well as self-tests INRs.
Novel Anticoagulants
Novel oral anticoagulants are administered in a fixed dose, establish effective anticoagulation within hours of administration, require no laboratory coagulation monitoring, and have few of the drug-drug or drug-food interactions that make warfarin so difficult to dose. Rivaroxaban, a factor Xa inhibitor, and dabigatran, a direct thrombin inhibitor, are approved in Canada and Europe for prevention of VTE after total hip and total knee replacement. In a large-scale trial of acute VTE treatment, dabigatran was as effective as warfarin and had less nonmajor bleeding. Because of these drugs’ rapid onset of action and relatively short half-life compared with warfarin, “bridging” with a parenteral anticoagulant is not required.
Complications of Anticoagulants
The most serious adverse effect of anticoagulation is hemorrhage. For life-threatening or intracranial hemorrhage due to heparin or LMWH, protamine sulfate can be administered. There is no specific antidote for bleeding caused by fondaparinux or direct thrombin inhibitors.
Major bleeding from warfarin is best managed with prothrombin complex concentrate. With non-life threatening bleeding in a patient who can tolerate large volume, fresh-frozen plasma can be used. Recombinant human coagulation factor VIIa (rFVIIa), FDA-approved for bleeding in hemophiliacs, is an off-label option to manage catastrophic bleeding from warfarin. For minor bleeding or to manage an excessively high INR in the absence of bleeding, oral vitamin K may be administered.
Heparin-induced thrombocytopenia (HIT) and osteopenia are far less common with LMWH than with UFH. Thrombosis due to HIT should be managed with a direct thrombin inhibitor: argatroban for patients with renal insufficiency and lepirudin for patients with hepatic failure. In the setting of percutaneous coronary intervention, one should administer bivalirudin.
During pregnancy, warfarin should be avoided if possible because of warfarin embryopathy, which is most common with exposure during the sixth through twelfth week of gestation. However, women can take warfarin postpartum and breast-feed safely. Warfarin can also be administered safely during the second trimester.
Duration of Hospital Stay
Acute DVT patients with good family and social support, permanent residence, telephone service, and no hearing or language impairment often can be managed as outpatients. They, a family member, or a visiting nurse must administer a parenteral anticoagulant. Warfarin dosing can be titrated to the INR and adjusted on an outpatient basis.
Acute PE patients, who traditionally have required hospital stays of 5–7 days for intravenous heparin as a “bridge” to warfarin, can be considered for abbreviated hospitalization if they have a reliable support system at home and an excellent prognosis. Criteria include clinical stability, absence of chest pain or shortness of breath, normal RV size and function, and normal levels of cardiac biomarkers.
Duration of Anticoagulation
Patients with PE after surgery, trauma, or estrogen exposure (from oral contraceptives, pregnancy, or postmenopausal therapy) ordinarily have a low rate of recurrence after 3–6 months of anticoagulation. For DVT isolated to an upper extremity or calf that has been provoked by surgery, trauma, estrogen, or an indwelling central venous catheter or pacemaker, 3 months of anticoagulation suffices. For provoked proximal leg DVT or PE, 3 to 6 months of anticoagulation is sufficient. For patients with cancer and VTE, the consensus is to prescribe 3–6 months of LMWH as monotherapy without warfarin and to continue anticoagulation indefinitely unless the patient is rendered cancer-free. However, there is uncertainty whether subsequent anticoagulation should continue with LMWH or whether the patient should be placed on warfarin.
Among patients with idiopathic, unprovoked VTE, the recurrence rate is high after cessation of anticoagulation. VTE that occurs during long-haul air travel is considered unprovoked. It appears that unprovoked VTE is often a chronic illness, with latent periods between flares of recurrent episodes. American College of Chest Physicians (ACCP) guidelines recommend considering anticoagulation for an indefinite duration with a target INR between 2 and 3 for patients with idiopathic VTE. An alternative approach after the first 6 months of anticoagulation is to reduce the intensity of anticoagulation and to lower the target INR range to between 1.5 and 2.
Counterintuitively, the presence of genetic mutations such as heterozygous factor V Leiden and prothrombin gene mutation do not appear to increase the risk of recurrent VTE. However, patients with moderate or high levels of anticardiolipin antibodies probably warrant indefinite-duration anticoagulation even if the initial VTE was provoked by trauma or surgery.
Inferior Vena Caval (IVC) Filters
The two principal indications for insertion of an IVC filter are (1) active bleeding that precludes anticoagulation and (2) recurrent venous thrombosis despite intensive anticoagulation. Prevention of recurrent PE in patients with right heart failure who are not candidates for fibrinolysis and prophylaxis of extremely high-risk patients are “softer” indications for filter placement. The filter itself may fail by permitting the passage of small- to medium-size clots. Large thrombi may embolize to the pulmonary arteries via collateral veins that develop. A more common complication is caval thrombosis with marked bilateral leg swelling.
Paradoxically, by providing a nidus for clot formation, filters double the DVT rate over the ensuing 2 years after placement. Retrievable filters can now be placed for patients with an anticipated temporary bleeding disorder or for patients at temporary high risk of PE, such as individuals undergoing bariatric surgery who have a prior history of perioperative PE. The filters can be retrieved up to several months after insertion unless thrombus forms and is trapped within the filter. The retrievable filter becomes permanent if it remains in place or if, for technical reasons such as rapid endothelialization, it cannot be removed.
Maintaining Adequate Circulation
For patients with massive PE and hypotension, one should administer 500 mL of normal saline. Additional fluid should be infused with extreme caution because excessive fluid administration exacerbates RV wall stress, causes more profound RV ischemia, and worsens LV compliance and filling by causing further interventricular septal shift toward the LV. Dopamine and dobutamine are first-line inotropic agents for treatment of PE-related shock. There should be a low threshold for initiating these pressors. Often, a “trial-and-error” approach works best; one should consider norepinephrine, vasopressin, or phenylephrine.
Fibrinolysis
Successful fibrinolytic therapy rapidly reverses right heart failure and may result in a lower rate of death and recurrent PE by (1) dissolving much of the anatomically obstructing pulmonary arterial thrombus, (2) preventing the continued release of serotonin and other neurohumoral factors that exacerbate pulmonary hypertension, and (3) lysing much of the source of the thrombus in the pelvic or deep leg veins, thereby decreasing the likelihood of recurrent PE.
The preferred fibrinolytic regimen is 100 mg of recombinant tissue plasminogen activator (tPA) administered as a continuous peripheral intravenous infusion over 2 hours. Patients appear to respond to fibrinolysis for up to 14 days after the PE has occurred.
Contraindications to fibrinolysis include intracranial disease, recent surgery, and trauma. The overall major bleeding rate is about 10%, including a 1–3% risk of intracranial hemorrhage. Careful screening of patients for contraindications to fibrinolytic therapy is the best way to minimize bleeding risk.
The only FDA-approved indication for PE fibrinolysis is massive PE. For patients with preserved systolic blood pressure and submassive PE with moderate or severe RV dysfunction, ACCP guidelines for fibrinolysis recommend individual patient risk assessment of the thrombotic burden versus the bleeding risk.
Pulmonary Embolectomy
The risk of intracranial hemorrhage with fibrinolysis has prompted a renaissance of surgical embolectomy. More prompt referral before the onset of irreversible cardiogenic shock and multisystem organ failure and improved surgical technique have resulted in a high survival rate. A possible alternative to open surgical embolectomy is catheter embolectomy. New-generation catheters are under development.
Pulmonary Thromboendarterectomy
Chronic thromboembolic pulmonary hypertension occurs in 2–4% of acute PE patients. Therefore, PE patients who have initial pulmonary hypertension (usually diagnosed with Doppler echocardiography) should be followed up at about 6 weeks with a repeat echocardiogram to determine whether pulmonary arterial pressure has normalized. Patients impaired by dyspnea due to chronic thromboembolic pulmonary hypertension should be considered for pulmonary thromboendarterectomy, which, if successful, can markedly reduce, and at times even cure, pulmonary hypertension . The operation requires median sternotomy, cardiopulmonary bypass, deep hypothermia, and periods of hypothermic circulatory arrest. The mortality rate at experienced centers is approximately 5%.
Emotional Support
Patients with VTE may feel overwhelmed when they learn that they are susceptible to recurrent PE or DVT. They worry about the health of their families and the genetic implications of their illness. Those who are advised to discontinue warfarin after 3–6 months of therapy may feel especially vulnerable. At Brigham and Woman’s Hospital a physican-nurse–facilitated PE support group has been maintained for patients and has met monthly for more than 15 years.
Prevention of Postphlebitic Syndrome
Daily use of below-knee 30- to 40-mmHg vascular compression stockings will halve the rate of developing postphlebitic syndrome. These stockings should be prescribed as soon as DVT is diagnosed and should be fitted carefully to maximize their benefit. When patients are in bed, the stockings need not be worn.
Prevention of VTE
Prophylaxis (Table L-5) is of paramount importance because VTE is difficult to detect and poses a profound medical and economic burden. Computerized reminder systems can increase the use of preventive measures and at Brigham and Women’s Hospital have reduced the symptomatic VTE rate by more than 40%. Patients who have undergone total hip or knee replacement or cancer surgery will benefit from extended pharmacologic prophylaxis for a total of 4–5 weeks.
Table L-5 Prevention of Venous Thromboembolism
| Condition | Prophylaxis Strategy |
| High-risk general surgery | Mini-UFH or LMWH |
| Thoracic surgery | Mini-UFH + IPC |
| Cancer surgery, including gynecologic cancer surgery | LMWH, consider 1 month of prophylaxis |
| Total hip replacement, total knee replacement, hip fracture surgery | LMWH, fondaparinux (a pentasaccharide) 2.5 mg SC, once daily, or (except for total knee replacement) warfarin (target INR 2.5); rivaroxaban or dalteparin in countries where it is approved |
| Neurosurgery | IPC |
| Neurosurgery for brain tumor | Mini-UFH or LMWH, + IPC + predischarge venous ultrasonography |
| Benign gynecologic surgery | Mini-UFH |
| Medically ill patients | Mini-UFH or LMWH |
| Anticoagulation contraindicated | IPC |
| Long-haul air travel | Consider LMWH for very high-risk patients |
 _U.S. Dollar
_U.S. Dollar _Nepali Rupees
_Nepali Rupees