
Obstructive Sleep Apnea
Obstructive sleep apnea or hypopnea syndrome (OSAHS) is one of the most important medical conditions identified in the last 50 years. It is a major cause of morbidity, a significant cause of mortality, and the most common medical cause of daytime sleepiness. Central sleep apnea is a rare clinical problem.
Definition
OSAHS is defined as the coexistence of unexplained excessive daytime sleepiness with at least five obstructed breathing events (apnea or hypopnea) per hour of sleep (Table O-1). This event threshold may have to be increased in the elderly. Apneas are defined in adults as breathing pauses lasting ≥10 s and hypopneas as events ≥10 s in which there is continued breathing but ventilation is reduced by at least 50% from the previous baseline during sleep. As a syndrome, OSAHS is the association of a clinical picture with specific abnormalities on testing; asymptomatic individuals with abnormal breathing during sleep should not be labeled as having OSAHS.
Table O-1 Clinical Indicators in the Sleepy Patient
| OSAHS | Narcolepsy | IHS | |
| Age of onset (years) | 35–60 | 10–30 | 10–30 |
| Cataplexy | No | Yes | No |
| Night sleep | |||
| Duration | Normal | Normal | Long |
| Awakenings | Occasional | Frequent | Rare |
| Snoring | Yes, loud | Occasional | Occasional |
| Morning drunkenness | Occasional | Occasional | Common |
| Daytime naps | |||
| Frequency | Usually few | Many | Few |
| Time of day | Afternoon/evening | Afternoon/evening | Morning |
| Duration | <1 h | <1 h | >1 h |
Mechanism of Obstruction
Apneas and hypopneas are caused by the airway being sucked closed on inspiration during sleep. This occurs as the upper-airway dilating muscles—like all striated muscles—relax during sleep. In patients with OSAHS, the dilating muscles fail to oppose negative pressure within the airway during inspiration. The primary defect is not in the upper-airway muscles, which function normally in OSAHS patients when awake. These patients have narrow upper airways already during wakefulness, but when they are awake, their airway dilating muscles have increased activity, which ensures airway patency. However, during sleep, muscle tone falls and the airway narrows; snoring may commence before the airway occludes, and apnea results. Apneas and hypopneas terminate when the subject arouses, i.e., wakens briefly, from sleep. This arousal is sometimes too subtle to be seen on the electroencephalogram but may be detected by cardiac acceleration, blood pressure elevation, or increase in sympathetic tone. The arousal results in return of upper-airway dilating muscle tone, and thus airway patency is resumed.
Factors predisposing to OSAHS by narrowing the pharynx include obesity—in Western populations around 50% of OSAHS patients have a body mass index (BMI) >30 kg/m2—and shortening of the mandible and/or maxilla. This change in jaw shape may be subtle and can be familial. Hypothyroidism and acromegaly predispose to OSAHS by narrowing the upper airway with tissue infiltration. Other predisposing factors for OSAHS include male sex and middle age (40–65 years), myotonic dystrophy, Ehlers-Danlos syndrome, and, perhaps, smoking.
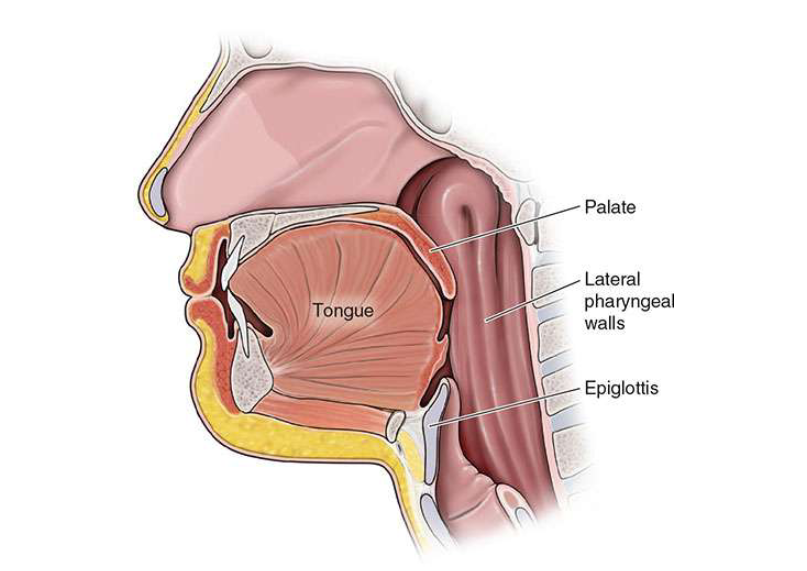
apnea include the palate, the tongue, and/or the epiglottis. In addition, collapse
can also occur due to the lateral pharyngeal walls.
Epidemiology
OSAHS occurs in around 1–4% of middle-aged males and is about half as common in women. The syndrome also occurs in childhood—usually associated with tonsil or adenoid enlargement—and in the elderly, although the frequency is slightly lower in old age. Irregular breathing during sleep without daytime sleepiness is much more common, occurring in perhaps a quarter of the middle-aged male population. As these individuals are asymptomatic, they do not have OSAHS, but there is increasing epidemiologic evidence of an association of irregular breathing during sleep with increased vascular risk even in the nonsleepy.
Clinical Features
Randomized controlled treatment trials have shown that OSAHS causes daytime sleepiness; impaired vigilance, cognitive performance and driving; depression; disturbed sleep; and hypertension. Daytime sleepiness may range from mild to irresistible and can be indistinguishable from that in narcolepsy. The sleepiness may cause inability to work effectively, damage interpersonal relationships, and prevent socializing. The somnolence is dangerous, with a three- to sixfold risk of road accidents. Experiments with normal subjects repeatedly aroused from sleep indicate that the sleepiness results, at least in part, from the repetitive sleep disruption associated with the breathing abnormality. Other symptoms include difficulty concentrating, unrefreshing nocturnal sleep, nocturnal choking, nocturia, and decreased libido. Partners report nightly loud snoring in all postures, which may be punctuated by the silence of apneas.
Cardiovascular and Cerebrovascular Events
OSAHS raises 24-h mean blood pressure. The increase is greater in those with recurrent nocturnal hypoxemia, is at least 4–5 mmHg, and may be as great as 10 mmHg in those with >20% arterial oxygen desaturations per hour of sleep. This rise probably results from a combination of surges in blood pressure accompanying each arousal at apnea/hypopnea termination and from the associated 24-h increases in sympathetic tone.
Epidemiologic data in normal populations indicate that this rise in blood pressure would increase the risk of myocardial infarction by around 20% and that of stroke by about 40%. Although there are no long-term randomized controlled trials to indicate whether this is true in OSAHS patients—such studies would be unethical—observational studies suggest an increase in cardiovascular and stroke risk in patients with untreated OSAHS. Furthermore, epidemiologic studies suggest increased vascular risk in normal subjects with raised apneas and hypopneas during sleep. Patients with recent stroke have a high frequency of apneas and hypopneas during sleep. These seem largely to be a consequence, not a cause, of the stroke and to decline over the weeks after the vascular event. There is no evidence that treating the apneas and hypopneas improves stroke outcome.
Diabetes Mellitus
The association of OSAHS with diabetes mellitus is not due only to the fact that obesity is common in both conditions. Increased apneas and hypopneas during sleep are associated with insulin resistance independent of obesity. In addition, uncontrolled trials suggest OSAHS can aggravate diabetes and that treating OSAHS in patients who also have diabetes decreases their insulin requirements.
Liver
Hepatic dysfunction also has been associated with irregular breathing during sleep. Non-alcohol-drinking subjects with apneas and hypopneas during sleep were found to have raised liver enzymes and more steatosis and fibrosis on liver biopsy, independent of body weight.
Anesthestic Risk
Patients with OSAHS are at increased risk perioperatively as their upper airways may obstruct during the recovery period or as a consequence of sedation. Patients whom anesthesiologists have difficulty intubating are much more likely to have irregular breathing during sleep. Anesthesiologists should thus take preoperative sleep histories and take the appropriate precautions with patients who might have OSAHS.
Differential Diagnosis
Causes of sleepiness that may need to be distinguished include (Table O-1) the following:
- Insufficient sleep: this usually can be diagnosed by history.
- Shift work: a major cause of sleepiness, especially in those >40 years old.
- Psychological psychiatric causes: depression is a major cause of sleepiness.
- Drugs: both stimulant and sedative drugs can produce sleepiness.
- Narcolepsy: around 50 times less common than OSAHS, narcolepsy is usually evident from childhood or the teens and is associated with cataplexy.
- Idiopathic hypersomnolence: this is an ill-defined condition typified by long sleep duration and sleepiness.
- Phase alteration syndromes: both the phase delay and the less common phase advancement syndromes are characterized by sleepiness at the appropriate time of day.
WHO to Refer for Diagnosis
Anyone whose troublesome sleepiness is not readily explained and rectified by considering the differential diagnosis above should be referred to a sleep specialist. The guideline the author uses for patients with troublesome sleepiness includes those with an Epworth Sleepiness Score >11 (Table O-2) and also those whose sleepiness during work or driving poses problems. The Epworth Score is not a perfect measure for detecting sleepiness, as many whose lives are troubled by frequently fighting sleepiness but who never doze will correctly give themselves a low Epworth Score. The patient and his or her partner often give divergent scores for the patient’s sleepiness, and in such cases the higher of the two scores should be used.
Table O-2 Epworth Sleepiness Score
| How often are you likely to doze off or fall asleep in the following situations, in contrast to feeling just tired? This refers to your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how they would have affected you. Use the following scale to choose the most appropriate number for each situation: |
| 0 = would never doze |
| 1 = slight chance of dozing |
| 2 = moderate chance of dozing |
| 3 = high chance of dozing |
| Sitting and reading ……………………………………….. |
| Watching TV ………………………………………… |
| Sitting, inactive in a public place (e.g., a theater or a meeting) ………………………………………… |
| As a passenger in a car for an hour without a break ………………………………………….. |
| Lying down to rest in the afternoon when circumstances permit ………………………………………….. |
| Sitting and talking to someone …………………………………………. |
| Sitting quietly after lunch without alcohol …………………………………………. |
| In a car, while stopped for a few minutes in traffic ………………………………………….. |
| TOTAL …………………………………………. |
Diagnosis
OSAHS requires lifelong treatment, and the diagnosis has to be made or excluded with certainty. This will hinge on obtaining a good sleep history from the patient and partner, with both completing sleep questionnaires, including the Epworth Sleepiness Score (Table O-2). Physical examination must include assessment of obesity, jaw structure, the upper airway, blood pressure, and possible predisposing causes, including hypothyroidism and acromegaly (see above).
In those with appropriate clinical features, the diagnostic test must demonstrate recurrent breathing pauses during sleep. This may be full polysomnography with recording of multiple respiratory and neurophysiologic signals during sleep. Increasingly, especially outside the United States, most diagnostic tests are “limited studies”—recording respiratory and oxygenation patterns overnight without neurophysiologic recording. Such approaches in expert hands produce good patient outcomes and are cost-effective. It is sensible to use such limited sleep studies as the first-line diagnostic test and then allow positively diagnosed patients to proceed to treatment. A reasonable approach at present is for patients with troublesome sleepiness but negative limited studies to have polysomnography to exclude or confirm OSAHS.
Treatment: Obstructive Sleep Apnea
Whom to Treat
There is evidence from robust randomized controlled trials (RCTs) that treatment improves symptoms, sleepiness, driving, cognition, mood, quality of life, and blood pressure in patients who have an Epworth Score >11, troublesome sleepiness while driving or working, and >15 apneas + hypopneas per hour of sleep. For those with similar degrees of sleepiness and 5–15 events per hour of sleep, RCTs indicate improvements in symptoms, including subjective sleepiness, with less strong evidence indicating gains in cognition and quality of life. There is no evidence of blood pressure improvements in this group. There is no robust evidence that treating nonsleepy subjects improves their symptoms, function, or blood pressure, and so treatment cannot be advocated for this large group, although this may change with further RCTs or less obtrusive therapy.
How to Treat
All patients diagnosed with OSAHS should have the condition and its significance explained to them and their partners. This should be accompanied by written and/or Web-based information and a discussion of the implications of the local driving regulations. Rectifiable predispositions should be discussed; this often includes weight loss and alcohol reduction both to reduce weight and because alcohol acutely decreases upper-airway dilating muscle tone, thus predisposing to obstructed breathing. Sedative drugs, which also impair airway tone, should be carefully withdrawn.
Continuous Positive Airway Pressure (CPAP)
CPAP therapy works by blowing the airway open during sleep, usually with pressures of 5–20 mmHg. CPAP has been shown in randomized placebo-controlled trials to improve breathing during sleep, sleep quality, sleepiness, blood pressure, vigilance, cognition, and driving ability as well as mood and quality of life in patients with OSAHS. However, this is obtrusive therapy, and care must be taken to explain the need for the treatment to patients and their partners and to intensively support patients on CPAP with telephone or Web support and regular follow-up. Initiation should include finding the most comfortable mask from the ranges of several manufacturers and trying the system for at least 30 min during the day to prepare for the overnight trial. An overnight monitored trial of CPAP is used to identify the pressure required to keep the patient’s airway patent. The development of pressure-varying CPAP machines has made an in-lab CPAP night trial unnecessary, but treatment must be initiated in a supportive environment. Thereafter, patients can be treated with fixed-pressure CPAP machines set at the determined pressure or with a self-adjusting intelligent CPAP device. The main side effect of CPAP is airway drying, which can be countered by using an integral heated humidifier. CPAP use is imperfect, but around 94% of patients with severe OSAHS are still using their therapy after 5 years on objective monitoring.
Mandibular Repositioning Splint (Mrs)
Also called oral devices, MRSs work by holding the lower jaw and the tongue forward, thereby widening the pharyngeal airway. MRSs have been shown in RCTs to improve OSAHS patients’ breathing during sleep, daytime somnolence, and blood pressure. As there are many devices with differing designs with unknown relative efficacy, these results cannot be generalized to all MRSs. Self-reports of the use of devices long-term suggest high dropout rates.
Surgery
Four forms of surgery have a role in OSAHS, although it must be remembered that these patients have a raised perioperative risk. Bariatric surgery can be curative in the morbidly obese. Tonsillectomy can be highly effective in children but rarely in adults. Tracheostomy is curative but rarely used because of the associated morbidity rate but should not be overlooked in severe cases. Jaw advancement surgery—particularly maxillomandibular osteotomy—is effective in those with retrognathia (posterior displacement of the mandible) and should be considered particularly in young and thin patients. There is no robust evidence that pharyngeal surgery, including uvulopalatopharyngoplasty (whether by scalpel, laser, or thermal techniques) helps OSAHS patients.
Drugs
Unfortunately, no drugs are clinically useful in the prevention or reduction of apneas and hypopneas. A marginal improvement in sleepiness in patients who remain sleepy despite CPAP can be produced by modafinil, but the clinical value is debatable and the financial cost is significant.
Choice of Treatment
CPAP and MRS are the two most widely used and best evidence-based therapies. Direct comparisons in RCTs indicate better outcomes with CPAP in terms of apneas and hypopneas, nocturnal oxygenation, symptoms, quality of life, mood, and vigilance. Adherence to CPAP is generally better than that to an MRS, and there is evidence that CPAP improves driving, whereas there are no such data on MRSs. Thus, CPAP is the current treatment of choice. However, MRSs are evidence-based second-line therapy in those who fail CPAP. In younger, thinner patients, maxillomandibular advancement should be considered.
Health Resources
Untreated OSAHS patients are heavy users of health care and dangerous drivers; they also work beneath their potential. Treatment of OSAHS with CPAP is cost-effective in terms of reducing the health care costs of associated illness and associated accidents.
Central Sleep Apnea
Central sleep apneas (CSAs) are respiratory pauses caused by lack of respiratory effort. They occur occasionally in normal subjects, particularly at sleep onset and in rapid eye movement (REM) sleep, and are transiently increased after ascent to altitude. Recurrent CSA is most commonly found in the presence of cardiac failure or neurologic disease, especially stroke. Spontaneous central sleep syndrome is rare and can be classified on the basis of the arterial Pco2.
Hypercapnic CSA occurs in conjunction with diminished ventilatory drive in Ondine’s curse (central alveolar hypoventilation). Patients with normocapnic spontaneous CSA have a normal or low arterial Pco2 when awake, with brisk ventilatory responses to hypercapnia. This combination results in unstable ventilatory control, with subjects breathing close to or below their apneic threshold for Pco2 during sleep; this apneic tendency is compounded by cycles of arousal-induced hyperventilation, inducing further hypocapnia.
Clinical Features
Patients may present with sleep maintenance insomnia, which is relatively unusual in OSAHS. Daytime sleepiness may occur.
Investigation
Many apneas previously labeled central because of absent thoracoabdominal movement are actually obstructive, identification of movement being particularly difficult in the very obese. CSA can be identified with certainty only if either esophageal pressure or respiratory muscle electromyography is recorded and shown to be absent during the events.
Treatment: Central Sleep Apnea
Patients with underlying cardiac failure should have their failure treated appropriately. CPAP may improve outcome but is difficult to initiate and has not been shown to improve survival. Patients with spontaneous normocapnic CSA may be treated with acetazolamide. In a minority of patients, CPAP is effective, perhaps because in some patients with OSAHS, pharyngeal collapse initiates reflex inhibition of respiration, and this is prevented by CPAP. Oxygen and nocturnal nasal positive-pressure ventilation also may be tried.
 _U.S. Dollar
_U.S. Dollar _Nepali Rupees
_Nepali Rupees