
Mitral valve prolapse is also called systolic click-murmur syndrome and floppy mitral valve syndrome. It’s probably a congenital abnormality.
Causes
- Autosomal dominant inheritance
- Inherited connective tissue disorders, such as Marfan syndrome, Ehlers-Danlos syndrome, and osteogenesis imperfecta
- Genetic or environmental interruption of valve development during week 5 or 6 of gestation
Pathophysiology
The cusps of the mitral valve are enlarged, thickened, and scalloped, possibly secondary to collagen abnormalities. The chordae tendineae may be longer than usual, allowing the cusps to stretch upward. Mitral regurgitation occurs when the valve permits blood to leak into the atrium.
Signs and symptoms
- Commonly produces no symptoms
- Late systolic regurgitant murmur
- Midsystolic click
- Palpitations, arrhythmias, tachycardia
- Light-headedness or syncope
- Fatigue, especially in the morning; lethargy; weakness
- Dyspnea, hyperventilation
- Chest tightness, atypical chest pain
- Anxiety, panic attacks, depression

Diagnostic test results
- Echocardiography reveals mitral valve prolapse with or without mitral insufficiency.
- Electrocardiography (resting and exercise) is usually normal but may show atrial or ventricular arrhythmia.
- Holter monitor detects arrhythmias.
Treatment
- Corresponds to degree of mitral regurgitation
- In the presence of regurgitation, antibiotic prophylaxis before invasive procedures to prevent infective endocarditis
- Beta-adrenergic blockers
- Measures to prevent hypovolemia, such as avoidance of diuretics, because hypervolemia can decrease ventricular volume, thereby increasing stress on the prolapsed mitral valve
- Surgical repair or valve replacement
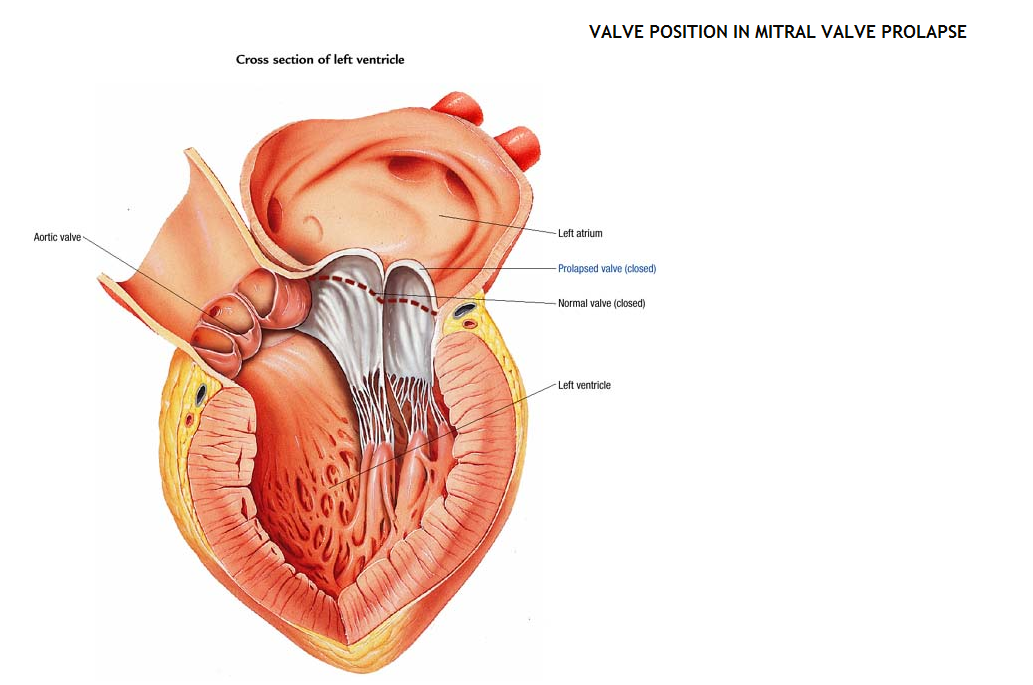
Fig: Valve position in mitral valve prolapse