
Fat embolism syndrome is a rare but potentially fatal problem. The syndrome involves pulmonary, cerebral, and cutaneous manifestations and occurs 24 to 48 hours postinjury.

Causes
- Fractures of the pelvis, femur, tibia, or ribs
- Orthopedic surgery
Pathophysiology
Bone marrow from a fractured bone or other injured adipose tissue releases fatty globules that enter the systemic circulation through torn veins at the injury site. These fatty globules travel to the lungs, where they form an embolus that blocks pulmonary circulation. Lipase breaks down the trapped fat emboli into free fatty acids.
This process causes a local toxic effect that damages the epithelium, increases capillary permeability, and inactivates lung surfactant. The increased capillary permeability allows protein-rich fluid to leak into the interstitial space and alveoli, increasing the workload of the right side of the heart and causing pulmonary edema. The decreased surfactant causes alveolar collapse, a decrease in functional reserve capacity, and ventilation-perfusion mismatch, leading to hypoxemia. Platelet aggregation on fat, normal injury-related platelet consumption, and platelet dilution through I.V. crystalloid administration all contribute to thrombocytopenia, petechiae and, possibly, disseminated intravascular coagulation.
Signs and symptoms
- Petechiae
- Increased respiratory rate
- Dyspnea
- Accessory muscle use
- Mental status changes
- Jaundice
- Fever
Treatment
- Supplemental oxygen
- Endotracheal intubation and mechanical ventilation
- I.V. fluids such as crystalloids (avoid colloids)
- Coughing and deep breathing
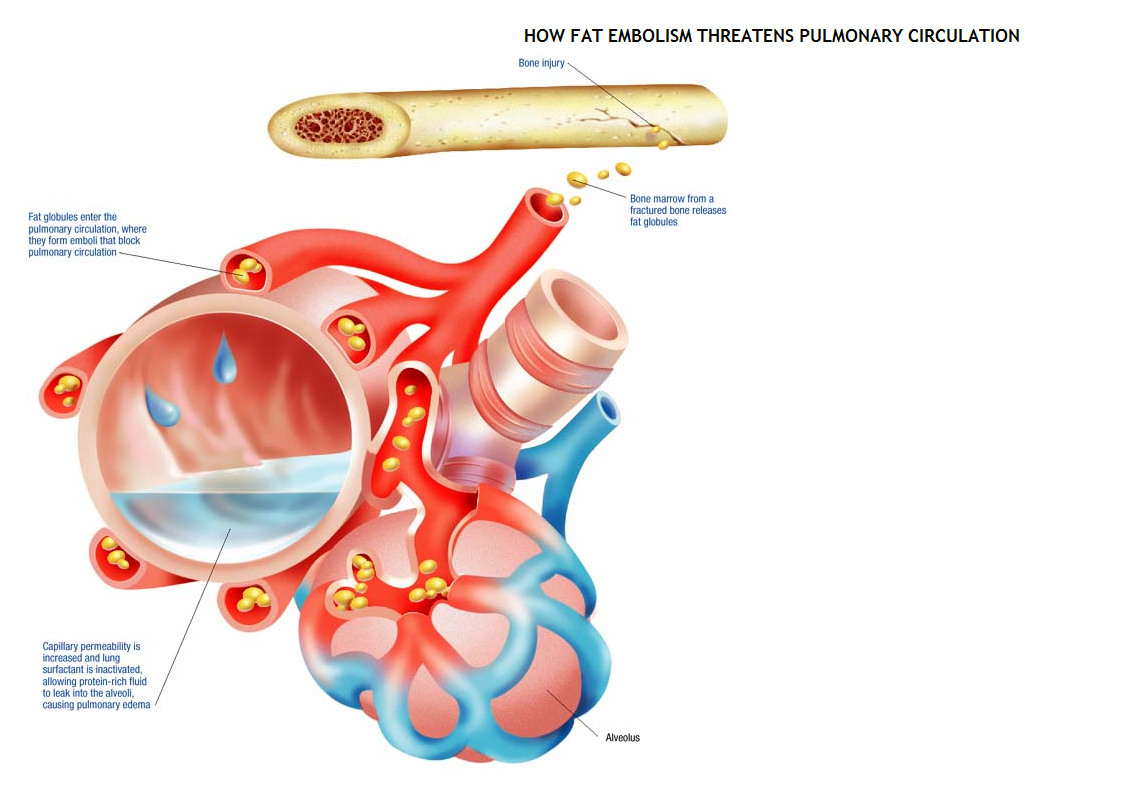
Fig: How fat embolism threatens pulmonary circulation