
| Medical Evaluation of the Surgical Patient |
Cardiovascular and pulmonary complications continue to account for major morbidity and mortality in patients undergoing noncardiac surgery. Emerging evidence-based practices dictate that the internist should perform an individualized evaluation of the surgical patient to provide an accurate preoperative risk assessment and stratification to guide optimum perioperative risk-reduction strategies. This chapter reviews cardiovascular and pulmonary preoperative risk assessment, targeting intermediate- and high-risk patients to strategically guide perioperative therapies to improve outcome. It also reviews perioperative management and prophylaxis of diabetes mellitus, endocarditis, and venous thromboembolism.
Anesthetics
Mortality is low with safe delivery of modern anesthesia, especially in low-risk patients undergoing low-risk surgery (Table 8-1). Inhaled anesthetics have predictable circulatory and respiratory effects; all decrease arterial pressure in a dose-dependent manner by reducing sympathetic tone, causing systemic vasodilation, myocardial depression, and decreased cardiac output. Inhaled anesthetics also cause respiratory depression with diminished responses to both hypercapnia and hypoxemia in a dose-dependent manner, and they have a variable effect on heart rate. In combination with neuromuscular blockade, inhaled anesthetic agents also cause reduction in functional residual lung capacity due to loss of diaphragmatic and intercostal muscle function. This decreases lung volume, which may lead to atelectasis in the dependent lung regions and, in turn, may result in arterial hypoxemia from ventilation-perfusion mismatch as well as an increased risk of postoperative pulmonary complications.
Table 8-1 Surgery: Gradation of Risk of Common Noncardiac Surgical Procedures
| Higher | •Emergent major operations, especially elderly •Aortic and other noncarotid major vascular surgery (endovascular and nonendovascular) •Prolonged surgery associated with large fluid shift and/or blood loss |
| Intermediate | •Major thoracic surgery •Major abdominal surgery •Carotid endarterectomy surgery •Head/neck surgery •Orthopedic surgery •Prostate surgery |
| Lower | •Eye, skin, and superficial surgery •Endoscopic procedures |
Several meta-analyses have shown that overall mortality was lower in patients receiving neuroaxial anesthesia (epidural or spinal) as compared to general (inhaled) anesthesia. Lower rates of venous thrombosis, pulmonary embolism, pneumonia, and respiratory depression were also observed in patients who were provided neuroaxial anesthesia; however, there were no significant differences in cardiac events between the two approaches. A combination of neuroaxial blockade and general anesthesia is useful when it is desired to reduce general anesthesia requirements. Evidence from a meta-analysis of randomized controlled trials also supports postoperative epidural analgesia for the purpose of pain relief for more than 24 h.
Evaluation of Intermediate- to High-Risk Patients
Simple, standardized preoperative screening questionnaires, such as the one shown in Table 8-2, have been developed for the purpose of identifying patients at intermediate or high risk who may benefit from a more detailed clinical evaluation. Evaluation of such patients for operation should always begin with a thorough history and physical examination and with a 12-lead resting ECG, in accordance with the American College of Cardiology/American Heart Association (ACC/AHA) guideline recommendations. The history should focus on symptoms of occult cardiac or pulmonary disease. The urgency of the surgery should be determined, as true emergency procedures are associated with an unavoidably higher morbidity and mortality. Preoperative laboratory testing should be carried out only for specific clinical conditions based on the clinical examination. Thus, healthy patients of any age undergoing elective surgical procedures without coexisting medical conditions should not require any testing unless the degree of surgical stress may result in unusual changes from the baseline state.
Table 8-2 Standardized Preoperative Questionnairesa
| 1. Age, weight, height |
| 2. Are you: |
| Female and 55 years of age or older or male and 45 years of age of older? |
| If yes, are you also 70 years of age or older? |
| 3. Do you take anticoagulant (“blood thinners”) medications? |
| 4. Do you have or have you had any of the following heart-related conditions? |
| Heart disease |
| Heart attack within the last six months |
| Angina (chest pain) |
| Irregular heartbeat |
| Heart failure |
| 5. Do you have or have you ever had any of the following? |
| Rheumatoid arthritis |
| Kidney disease |
| Liver disease |
| Diabetes |
| 6. Do you get short of breath when you lie flat? |
| 7. Are you currently on oxygen treatment? |
| 8. Do you have a chronic cough that produces any discharge or fluid? |
| 9. Do you have lung problems or diseases? |
| 10. Have you or any blood member of your family ever had a problem with any anesthesia other than nausea? |
| If yes, describe: |
| 11. If female, is it possible that you could be pregnant? |
| Pregnancy test: |
| Please list date of last menstrual period: |
Preoperative Cardiac Risk Assessment
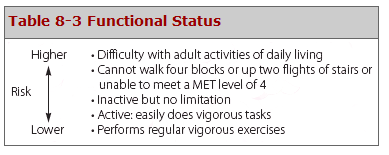
Assessment of exercise tolerance in the prediction of in-hospital perioperative risk is most helpful in patients who self-report worsening, exercise-induced cardiopulmonary symptoms; those who may benefit from noninvasive or invasive cardiac testing regardless of scheduled surgical procedure; and those with known coronary artery disease (CAD) or with multiple risk factors who are able to exercise. For predicting perioperative events, poor exercise tolerance has been defined as the inability to walk four blocks or climb two flights of stairs at a normal pace or to meet a metabolic equivalent (MET) level of four (e.g., carrying objects of 15–20 lb or playing golf or doubles tennis) because of the development of dyspnea, angina, or excessive fatigue (Table 8-3).
Previous studies have prospectively compared several cardiac risk indices. Given its accuracy and simplicity, the revised cardiac risk index (RCRI) (Table 8-4) is favored. The RCRI relies on the presence or absence of six identifiable predictive factors, which include high-risk surgery, ischemic heart disease, congestive heart failure, cerebrovascular disease, diabetes mellitus, and renal dysfunction. Each of these predictors is assigned one point. The risk of major cardiac events—defined as myocardial infarction, pulmonary edema, ventricular fibrillation or primary cardiac arrest, and complete heart block—can then be predicted. Based on the presence of none, one, two, three, or more of these clinical predictors, the rate of development of one of these major cardiac events is estimated to be 0.5, 1, 5, and 10%, respectively (Fig. 8-1). RCRI 0 has 0.4–0.5% risk of cardiac events; RCRI 1 has 0.9–1.3%; RCRI 2 has 4–6.6%; and RCRI ≥3 has 9–11% risk of cardiac events. The clinical utility of the RCRI is to identify patients with three or more predictors who are at higher risk (≥10%) for cardiac complications and who may benefit from further risk stratification with noninvasive cardiac testing or initiation of preoperative preventive medical management.
| Table 8-4 Revised Cardiac Risk Index Clinical Markers |
| High-risk surgical procedures |
| Vascular surgery |
| Major intraperitoneal or intrathoracic procedures |
| Ischemic heart disease |
| History of myocardial infarction |
| Current angina considered to be ischemic |
| Requiring sublingual nitroglycerin |
| Positive exercise test |
| Pathological Q-waves on ECG |
| History of PTCA and/or CABG with current angina considered to be ischemic |
| Congestive heart failure |
| Left ventricular failure by physical examination |
| History of paroxysmal nocturnal dyspnea |
| History of pulmonary edema |
| S3 gallop on cardiac auscultation |
| Bilateral rales on pulmonary auscultation |
| Pulmonary edema on chest x-ray |
| Cerebrovascular disease |
| History of transient ischemic attack |
| History of cerebrovascular accident |
| Diabetes mellitus |
| Treatment with insulin |
| Chronic renal insufficiency |
| Serum creatinine >2 mg/dL |
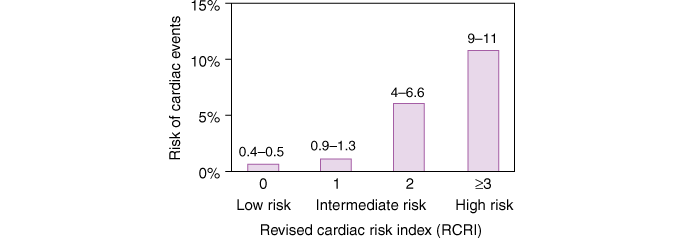
Risk stratification based on the RCRI. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Cardiac events include myocardial infarction, pulmonary edema, ventricular fibrillation, cardiac asystole, and complete heart block.
Preoperative Noninvasive Cardiac Testing for Risk Stratification
There is little evidence to support widespread application of preoperative noninvasive cardiac testing for all patients undergoing major surgery. Rather, a discriminate approach based on clinical risk categorization appears to be both useful clinically and cost-effective. There is potential benefit in identifying asymptomatic but high-risk patients, such as those with left main or left main–equivalent CAD or those with three-vessel CAD with poor left ventricular function who may benefit from coronary revascularization . However, evidence does not support aggressive attempts to identify patients at intermediate risk with asymptomatic but advanced coronary artery disease, because coronary revascularization appears to offer little advantage over medical therapy.
An RCRI score ≥3 in patients with severe myocardial ischemia on stress testing should lead to consideration of coronary revascularization prior to noncardiac surgery. Noninvasive cardiac testing is most appropriate if it is anticipated that in the event of a strongly positive test a patient will meet guidelines for coronary angiography and coronary revascularization. Pharmacologic stress tests are more useful than exercise testing in patients with functional limitations. Dobutamine echocardiography and persantine, adenosine, or dobutamine nuclear perfusion testing have excellent negative predictive values (near 100%) but poor positive predictive values (< 20%) for identification of patients at risk for perioperative myocardial infarction or death. Thus, a negative study is reassuring, but a positive study is a relatively weak predictor of a “hard” perioperative cardiac event. A stepwise approach is illustrated in Fig. 8-2.

Composite algorithm for cardiac risk assessment and stratification in patients undergoing noncardiac surgery. Stepwise clinical evaluation: [1] Emergency surgery; [2] Prior coronary revascularization; [3] Prior coronary evaluation; [4] Clinical assessment; [5] RCRI; [6] Risk modification strategies. Preventative medical therapy = beta blocker and statin therapy. RCRI, revised cardiac risk index.
Risk Modification Using Preventive Strategies to Reduce Cardiac Risk
Perioperative Coronary Revascularization
Currently, potential options for reducing perioperative cardiovascular risk include coronary artery revascularization and/or perioperative medical preventive therapies. Prophylactic coronary revascularization with either coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) provides no short- or midterm survival benefit for patients without left main CAD or three-vessel CAD in the presence of poor left ventricular systolic function. Although PCI is associated with lower procedural risk than is CABG in the perioperative setting, the placement of a coronary artery stent in a short period of time prior to noncardiac surgery may increase the risk of bleeding during surgery if dual antiplatelet therapy (aspirin and thienopyridine) is administered or it increases the perioperative risk of myocardial infarction and cardiac death due to stent thrombosis if such therapy is withdrawn prematurely. It is recommended that, if possible, noncardiac surgery be delayed 30–45 days after placement of a bare metal coronary stent and 365 days after a drug-eluting stent. For patients who must undergo noncardiac surgery early (> 14 days) after PCI, balloon angioplasty without stent placement appears to be a reasonable alternative because dual antiplatelet therapy is not necessary in such patients.
Perioperative Medical Preventive Therapies
Perioperative preventive medical therapy with β-adrenergic antagonists, HMG-CoA reductase inhibitors (statins), and aspirin have the goal of reducing perioperative adrenergic stimulation, ischemia, and inflammation, which are triggered during the perioperative period.
β-Adrenergic Antagonists
The use of perioperative beta blockade should be based on a thorough assessment of a patient’s perioperative cardiac risk (RCRI ≥ 2). For patients with or without mild to moderate reactive airway disease, the cardioselective beta blocker of choice should be used and titrated to a target resting heart rate of 60–65 beats/minute. In intermediate- to high-risk patients without a long-term indication for beta blockers, the medications can be administered intravenously as a preoperative medication on the day of surgery, with a targeted heart rate of 60–65 beats/minute and continued for > 7 days (preferably 30 days) postoperatively. Intravenous preparations should be substituted for oral medication if patients are unable to take or absorb pills in the perioperative period. The results from the recent Perioperative Ischemic Evaluation (POISE) trial showed that although cardiac death, nonfatal myocardial infarction, or cardiac arrest was reduced in the patients who received metoprolol as compared to placebo, there was an increased incidence of mortality and stroke in the patients receiving metoprolol because of a high and rapid loading dose of metoprolol. The POISE trial highlights the importance for a clear risk and benefit assessment with careful initiation and titration to therapeutic efficacy of preoperative beta blockers in patients undergoing noncardiac surgery.
The ACC/AHA guidelines recommend the following: (1) Beta blockers should be continued in high-risk patients who previously received these drugs and undergo vascular surgery, and they should be administered to high-risk patients identified by myocardial ischemia on preoperative assessment who are scheduled to undergo vascular surgery. (2) Beta blockers are probably recommended for high-risk patients defined by multiple clinical predictors who undergo intermediate- or high-risk procedures. They may be considered for intermediate-risk patients who undergo intermediate- or high-risk procedures and for low-risk patients who undergo vascular surgery.
HMG-CoA Reductase Inhibitors (Statins)
A number of prospective and retrospective studies support the perioperative prophylactic use of statins for reduction of cardiac complications in patients with established atherosclerosis. The Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE)-IV study, in addition to confirming the benefit of perioperative bisoprolol in lowering the risk of cardiac death or myocardial infarction at 30 days, demonstrated a reduced trend in cardiac events in intermediate-risk patients undergoing noncardiac surgery who receive fluvastatin therapy. The use of perioperative statin therapy to reduce perioperative cardiac risk should, therefore, be considered in intermediate- or high-risk patients with atherosclerotic cardiovascular disease who are undergoing major noncardiac surgery.
Angiotensin-Converting Enzyme (ACE) Inhibitors
Evidence supports the discontinuation of ACE inhibitors and angiotensin receptor blockers for 24 hours prior to noncardiac surgery due to adverse circulatory effects after induction of anesthesia.
Oral Antiplatelet Agents
Evidence-based recommendations regarding perioperative use of aspirin and/or thienopyridine to reduce cardiac risk currently lack clarity. A substantial increase in perioperative bleeding and transfusion requirement in patients receiving dual antiplatelet therapy has been observed. The discontinuation of thienopyridine and aspirin for 5–7 days prior to major surgery to minimize the risk of perioperative bleeding and transfusion must be balanced with the potential increased risk of an acute coronary syndrome and of subacute stent thrombosis in patients with recent coronary stent implantation. If clinicians elect to withhold antiplatelet agents prior to surgery, they should be restarted as soon as possible postoperatively.
Calcium Channel Blockers
Evidence is lacking to support the use of calcium channel blockers as a prophylactic strategy to decrease perioperative risk in major noncardiac surgery.
Preoperative Pulmonary Assessment
Perioperative pulmonary complications occur frequently and lead to significant morbidity and mortality. The guidelines from the American College of Physicians recommend the following:
- All patients undergoing noncardiac surgery should be assessed for risk of pulmonary complications (Table 8-5).
- Patients undergoing emergency or prolonged (>3 h) surgery; aortic aneurysm repair; vascular surgery; major abdominal, thoracic, neuro, head, or neck surgery; and general anesthesia should be considered to be at higher risk for postoperative pulmonary complications.
- Patients at higher risk of pulmonary complications should receive deep breathing exercises and/or incentive spirometry as well as selective use of a nasogastric tube for postoperative nausea, vomiting, or symptomatic abdominal distention to reduce postoperative risk (Table 8-6).
- Routine preoperative spirometry and chest radiography are less helpful for predicting risk of postoperative pulmonary complications, but may be appropriate for patients with chronic obstructive pulmonary disease (COPD) or asthma.
- Pulmonary artery catheterization, total parenteral nutrition, and total enteral nutrition are not encouraged for postoperative pulmonary risk reduction.
| Table 8-5 Predisposing Risk Factors for Pulmonary Complications |
| 1. Upper respiratory tract infection: cough, dyspnea |
| 2. Age >60 years |
| 3. COPD |
| 4. American Society of Anesthesiologists Class ≥2 |
| 5. Functionally dependent |
| 6. Congestive heart failure |
| 7. Serum albumin <3.5 g/dL |
| 8. FEV1<2 L |
| 9. MVV <50% of predicted |
| 10. PEF <100 L or 50% predicted value |
| 11. PCO2≥45 mmHg |
| 12. PO2≤50 mmHg |
| Table 8-6 Risk Modification to Reduce Perioperative Pulmonary Complications |
| Preoperatively ▪ Cessation of smoking ▪ Training in proper breathing (incentive spirometry) ▪ Inhalation bronchodilator therapy ▪ Control of infection and secretion, when indicated ▪ Weight reduction, when appropriate |
| Intraoperatively ▪ Limited duration of anesthesia ▪ Select shorter acting neuromuscular blocking drugs when indicated ▪ Prevention of aspiration ▪ Maintenance of optimal bronchodilation |
| Postoperatively ▪Continuation of preoperative measures, with particular attention to inspiratory capacity maneuvers mobilization of secretions early ambulation encouragement of coughing selective use of a nasogastric tube adequate pain control without excessive narcotics |
Other Preoperative Pulmonary Risk-Modification Strategies
Risk-modification strategies to reduce postoperative pulmonary complications should be implemented, particularly in higher-risk patients. Patients with cough or dyspnea preoperatively should be evaluated to determine the underlying cause of these symptoms. Patients who smoke should be counseled to quit for at least eight weeks prior to elective surgery. Patients with asthma or COPD can be given steroids and bronchodilators pre- and postoperatively to optimize pulmonary function. Bacterial pulmonary infection should be treated preoperatively.
Diabetes Mellitus
Many patients with diabetes mellitus have significant symptomatic or asymptomatic CAD and may have silent myocardial ischemia due to autonomic dysfunction. Evidence supports intensive perioperative glycemic control to achieve near-normal glucose levels (90–110 mg/dL) versus moderate glycemic control (120–200 mg/dL), using insulin infusion. This practice must be balanced against the risk of hypoglycemic complications. Oral hypoglycemic agonists should be held on the morning of operation. Perioperative hyperglycemia should be treated with intravenous infusion of short-acting insulin or subcutaneous sliding-scale insulin. Patients who are diet-controlled may proceed to surgery with close postoperative monitoring.
Prophylaxis for Infective Endocarditis
Perioperative prophylactic antibiotics should be administered to patients with congenital or valvular heart disease, prosthetic valves, mitral valve prolapse, or other cardiac abnormalities in accordance with ACC/AHA practice guidelines.
Prophylaxis of Venous Thromboembolism
Perioperative prophylaxis of venous thromboembolism should follow established guidelines of the American College of Chest Physicians. Aspirin is not supported as a single agent for thromboprophylaxis. Low-dose unfractionated heparin (≤5000 units subcutaneous bid), low-molecular weight heparin (e.g., enoxaparin 30 mg bid or 40 mg qd) or a pentasaccharide (fondaparinux 2.5 mg qd) for patients at moderate risk, and unfractionated heparin (5000 units subcutaneous tid) for patients at high risk. Graduated compression stockings and pneumatic compression devices are useful supplements to anticoagulant therapy.