
Occupational and Environmental Lung Disease: Introduction
Occupational and environmental lung diseases are difficult to distinguish from those of nonenvironmental origin. Virtually all major categories of pulmonary disease can be caused by environmental agents, and environmentally related disease usually presents clinically in a manner indistinguishable from that of disease not caused by such agents. In addition, the etiology of many diseases may be multifactorial; occupational and environmental factors may interact with other factors (such as smoking and genetic risk). It is often only after a careful exposure history is taken that the underlying workplace or general environmental exposure is uncovered.
Why is knowledge of occupational or environmental etiology so important? Patient management and prognosis are affected significantly by such knowledge. For example, patients with occupational asthma or hypersensitivity pneumonitis often cannot be managed adequately without cessation of exposure to the offending agent. Establishment of cause may have significant legal and financial implications for a patient who no longer can work in his or her usual job. Other exposed people may be identified as having the disease or prevented from getting it. In addition, new associations between exposure and disease may be identified (e.g., nylon flock worker’s lung disease and diacetyl-induced bronchiolitis obliterans).
Although the exact proportion of lung disease due to occupational and environmental factors is unknown, a large number of individuals are at risk. For example, 15–20% of the burden of adult asthma and chronic obstructive pulmonary disease (COPD) has been estimated to be due to occupational factors.
History and Physical Examination
The patient’s history is of paramount importance in assessing any potential occupational or environmental exposure. Inquiry into specific work practices should include questions about the specific contaminants involved, the presence of visible dusts, chemical odors, the size and ventilation of workspaces, the use of respiratory protective equipment, and whether co-workers have similar complaints. The temporal association of exposure at work and symptoms may provide clues to occupation-related disease. In addition, the patient must be questioned about alternative sources of exposure to potentially toxic agents, including hobbies, home characteristics, exposure to secondhand smoke, and proximity to traffic or industrial facilities. Short-term and long-term exposures to potential toxic agents in the distant past also must be considered.
Workers in the United States have the right to know about potential hazards in their workplaces under federal Occupational Safety and Health Administration (OSHA) regulations. Employers must provide specific information about potential hazardous agents in products being used through Material Safety Data Sheets as well as training in personal protective equipment and environmental control procedures. Reminders posted in the workplace may warn workers about hazardous substances. However, the introduction of new processes and/or new chemical compounds may change exposure significantly, and often only the employee on the production line is aware of the change. For the physician caring for a patient with a suspected work-related illness, a visit to the work site can be very instructive. Alternatively, an affected worker can request an inspection by OSHA.
The physical examination of patients with environmentally related lung diseases may help determine the nature and severity of the pulmonary condition but usually does not contribute information that points to a specific etiology.
Pulmonary Function Tests and Chest Imaging
Exposures to inorganic and organic dusts can cause interstitial lung disease that presents with a restrictive pattern and a decreased diffusing capacity. Similarly, exposures to a number of organic dusts or chemical agents may result in occupational asthma or COPD that is characterized by airway obstruction. Measurement of change in forced expiratory volume (FEV1) before and after a working shift can be used to detect an acute bronchoconstrictive response. For example, an acute decrement of FEV1 over the first work shift of the week is a characteristic feature of cotton textile workers with byssinosis (an obstructive airway disorder with features of both asthma and chronic bronchitis).
The chest radiograph is useful in detecting and monitoring the pulmonary response to mineral dusts, certain metals, and organic dusts capable of inducing hypersensitivity pneumonitis. The International Labour Organisation (ILO) International Classification of Radiographs of Pneumoconioses classifies chest radiographs by the nature and size of opacities seen and the extent of involvement of the parenchyma. In general, small rounded opacities are seen in silicosis or coal worker’s pneumoconiosis and small linear opacities are seen in asbestosis. The profusion of such opacities is rated by using a 12-point scheme. Although useful for epidemiologic studies and screening large numbers of workers, the ILO system can be problematic when applied to an individual worker’s chest radiograph. With dusts causing rounded opacities, the degree of involvement on the chest radiograph may be extensive, whereas pulmonary function may be only minimally impaired. In contrast, in pneumoconiosis causing linear, irregular opacities like those seen in asbestosis, the radiograph may lead to underestimation of the severity of the impairment until relatively late in the disease. For patients with a history of asbestos exposure, conventional computed tomography (CT) is more sensitive for the detection of pleural thickening and high-resolution CT (HRCT) improves the detection of asbestosis.
Other procedures that may be of use in identifying the role of environmental exposures in causing lung disease include evaluation of heavy metal concentrations in urine (cadmium in battery plant workers), skin prick testing or specific IgE antibody titers for evidence of immediate hypersensitivity to agents capable of inducing occupational asthma (flour antigens in bakers), specific IgG precipitating antibody titers for agents capable of causing hypersensitivity pneumonitis (pigeon antigen in bird handlers), and assays for specific cell-mediated immune responses (beryllium lymphocyte proliferation testing in nuclear workers or tuberculin skin testing in health care workers). Sometimes a bronchoscopy to obtain transbronchial biopsies of lung tissue may be required for histologic diagnosis (chronic beryllium disease). Rarely, video-assisted thoracoscopic surgery to obtain a larger sample of lung tissue may be required to determine the specific diagnosis of environmentally induced lung disease (hypersensitivity pneumonitis or giant cell interstitial pneumonitis due to cobalt exposure).
Exposure Assessment
If reliable environmental sampling data are available, that information should be used in assessing a patient’s exposure. Since many of the chronic diseases result from exposure over many years, current environmental measurements should be combined with work histories to arrive at estimates of past exposure.
In situations in which individual exposure to specific agents—either in a work setting or via ambient air pollutants—has been determined, the chemical and physical characteristics of those agents affect both the inhaled dose and the site of deposition in the respiratory tract. Water-soluble gases such as ammonia and sulfur dioxide are absorbed in the lining fluid of the upper and proximal airways and thus tend to produce irritative and bronchoconstrictive responses. In contrast, nitrogen dioxide and phosgene, which are less soluble, may penetrate to the bronchioles and alveoli in sufficient quantities to produce acute chemical pneumonitis that can be life-threatening.
Particle size of air contaminants must also be considered. Because of their settling velocities in air, particles >10–15 micro-meter in diameter do not penetrate beyond the nose and throat. Particles <10 micro-meter in size are deposited below the larynx. These particles are divided into three size fractions on the basis of their size characteristics and sources. Particles ~2.5–10 micro-meter (coarse-mode fraction) contain crustal elements such as silica, aluminum, and iron. These particles mostly deposit relatively high in the tracheobronchial tree. Although the total mass of an ambient sample is dominated by these larger respirable particles, the number of particles, and therefore the surface area on which potential toxic agents can deposit and be carried to the lower airways, is dominated by particles <2.5 micro-meter (fine-mode fraction). These fine particles are created primarily by the burning of fossil fuels or high-temperature industrial processes resulting in condensation products from gases, fumes, or vapors. The smallest particles, those <0.1 micro-meter in size, represent the ultrafine fraction and make up the largest number of particles; they tend to remain in the airstream and deposit in the lung only on a random basis as they come into contact with the alveolar walls. If they do deposit, however, particles of this size range may penetrate into the circulation and be carried to extrapulmonary sites. New technologies create particles of this size (“nanoparticles”) for use in many commercial applications. Besides the size characteristics of particles and the solubility of gases, the actual chemical composition, mechanical properties, and immunogenicity or infectivity of inhaled material determine in large part the nature of the diseases found among exposed persons.
Occupational Exposures and Pulmonary Disease
Table H-1 provides broad categories of exposure in the workplace and diseases associated with chronic exposure in those industries.
| Table H-1 Categories of Occupational Exposure and Associated Respiratory Conditions |
| Occupational Exposures | Nature of Respiratory Responses | Comment |
| Inorganic Dusts | Inorganic Dusts | Inorganic Dusts |
| Asbestos: mining, processing, construction, ship repair | Fibrosis (asbestosis), pleural disease, cancer, mesothelioma | Virtually all new mining and construction with asbestos done in developing countries |
| Silica: mining, stone cutting, sandblasting, quarrying | Fibrosis (silicosis), progressive massive fibrosis (PMF), cancer, tuberculosis, chronic obstructive pulmonary disease (COPD) | Improved protection in United States, persistent risk in developing countries |
| Coal dust: mining | Fibrosis (coal worker’s pneumoconiosis), PMF, COPD | Risk persists in certain areas of United States, increasing in countries where new mines open |
| Beryllium: processing alloys for high-tech industries | Acute pneumonitis (rare), chronic granulomatous disease, lung cancer (highly suspect) | Risk in high-tech industries persists |
| Other metals: aluminum, chromium, cobalt, nickel, titanium, tungsten carbide, or “hard metal” (contains cobalt) | Wide variety of conditions from acute pneumonitis to lung cancer and asthma | New diseases appear with new process development |
| Organic Dusts | Organic Dusts | Organic Dusts |
| Cotton dust: milling, processing | Byssinosis (an asthma-like syndrome), chronic bronchitis, COPD | Increasing risk in developing countries with drop in United States as jobs shift overseas |
| Grain dust: elevator agents, dock workers, milling, bakers | Asthma, chronic bronchitis, COPD | Risk shifting more to migrant labor pool |
| Other agricultural dusts: fungal spores, vegetable products, insect fragments, animal dander, bird and rodent feces, endotoxins, microorganisms, pollens | Hypersensitivity pneumonitis (farmer’s lung), asthma, chronic bronchitis | Important in migrant labor pool but also resulting from in-home exposures |
| Toxic chemicals: wide variety of industries, see Table H-2 | Asthma, chronic bronchitis, COPD, hypersensitivity pneumonitis, pneumoconiosis, and cancer | Reduced risk with recognized hazards; increasing risk for developing countries where controlled labor practices are less stringent |
| Other respiratory environmental agents: uranium and radon daughters, secondhand tobacco smoke, polycyclic hydrocarbons, biomass smoke, diesel exhaust, welding fumes, wood finishing | Occupational exposures estimated to contribute to up to 10% of all lung cancers; chronic bronchitis, COPD, and fibrosis | In-home exposures important; in developing countries biomass smoke is a major risk factor for COPD among women |
Asbestos-Related Diseases
Asbestos is a generic term for several different mineral silicates, including chrysolite, amosite, anthophyllite, and crocidolite. In addition to workers involved in the production of asbestos products (mining, milling, and manufacturing), many workers in the shipbuilding and construction trades, including pipe fitters and boilermakers, were occupationally exposed because asbestos was widely used during the twentieth century for its thermal and electrical insulation properties. Asbestos also was used in the manufacture of fire-resistant textiles, in cement and floor tiles, and in friction materials such as brake and clutch linings.
Exposure to asbestos is not limited to persons who directly handle the material. Cases of asbestos-related diseases have been encountered in individuals with only bystander exposure, such as painters and electricians who worked alongside insulation workers in a shipyard. Community exposure resulted from the use of asbestos-containing mine and mill tailings as landfill, road surface, and playground material (e.g., Libby, MT, the site of a vermiculite mine in which the ore was contaminated with asbestos). Finally, exposure can occur from the disturbance of naturally occurring asbestos (e.g., from increasing residential development in the foothills of the Sierra Mountains in California).
Asbestos has largely been replaced in the developed world with synthetic mineral fibers such as fiberglass and refractory ceramic fibers, but it continues to be used increasingly in the developing world. Despite current OSHA regulations mandating adequate training for any worker potentially exposed to asbestos, exposure continues among inadequately trained and protected demolition workers. The major health effects from exposure to asbestos are pleural and pulmonary fibrosis, cancers of the respiratory tract, and pleural and peritoneal mesothelioma.
Asbestosis is a diffuse interstitial fibrosing disease of the lung that is directly related to the intensity and duration of exposure. The disease resembles other forms of diffuse interstitial fibrosis . Usually, moderate to severe exposure has taken place for at least 10 years before the disease becomes manifest, and it may occur after exposure to any of the asbestiform fiber types. The mechanisms by which asbestos fibers induce lung fibrosis are not completely understood but are known to involve oxidative injury due to the generation of reactive oxygen species by the transition metals on the surface of the fibers as well as from cells engaged in phagocytosis.
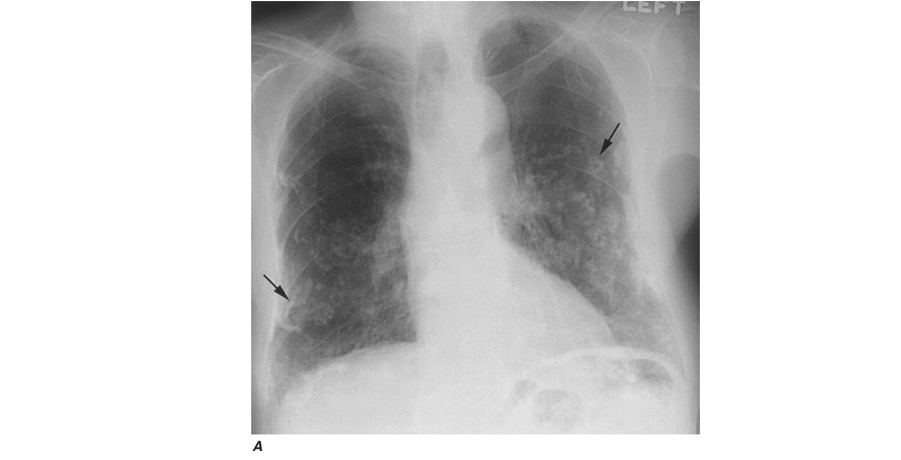
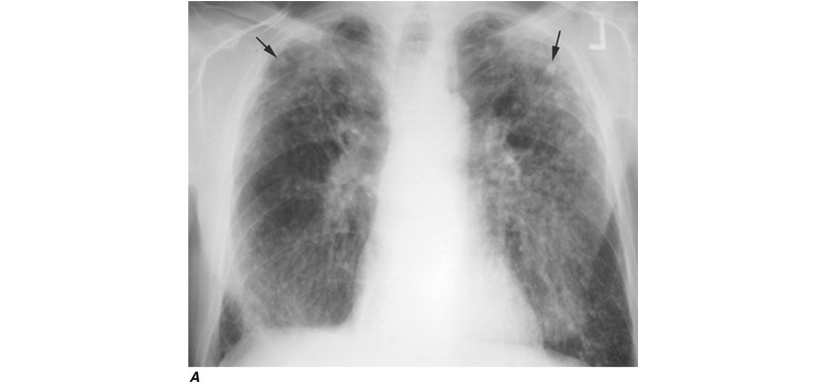
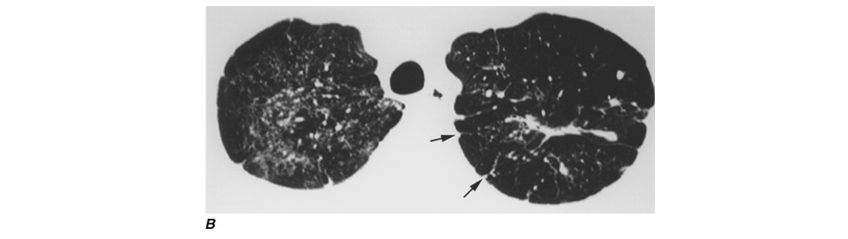
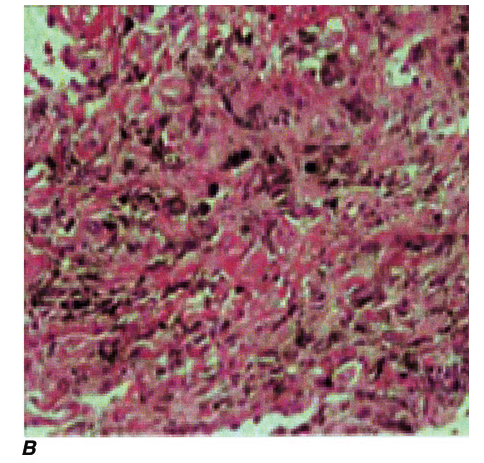
The chest radiograph can be used to detect the pulmonary manifestations of asbestos exposure. Past exposure is specifically indicated by pleural plaques, which are characterized by either thickening or calcification along the parietal pleura, particularly along the lower lung fields, the diaphragm, and the cardiac border. Without additional manifestations, pleural plaques imply only exposure, not pulmonary impairment. Benign pleural effusions also may occur. The fluid is typically a serous or bloody exudate. The effusion may be slowly progressive or may resolve spontaneously. Irregular or linear opacities, evidence of asbestosis that usually are first noted in the lower lung fields and spreading into the middle and upper lung fields, occur as the disease progresses. An indistinct heart border or a “ground-glass” appearance in the lung fields is seen in some cases. In cases in which the x-ray changes are less obvious, HRCT may show distinct changes of subpleural curvilinear lines 5–10 mm in length that appear to be parallel to the pleural surface (Fig. H-1).

Pulmonary function testing in asbestosis reveals a restrictive pattern with a decrease in both lung volumes and diffusing capacity. There may also be evidence of mild airflow obstruction (due to peribronchiolar fibrosis).
No specific therapy is available for the management of patients with asbestosis. The supportive care is the same as that given to any patient with diffuse interstitial fibrosis of any cause. In general, newly diagnosed cases will have resulted from exposures that occurred many years before.
Lung cancer is the most common cancer associated with asbestos exposure. The excess frequency of lung cancer (all histologic types) in asbestos workers is associated with a minimum latency of 15–19 years between first exposure and development of the disease. Persons with more exposure are at greater risk of disease. In addition, there is a significant interactive effect of smoking and asbestos exposure that results in greater risk than what would be expected from the additive effect of each factor.
Mesotheliomas , both pleural and peritoneal, are also associated with asbestos exposure. In contrast to lung cancers, these tumors do not appear to be associated with smoking. Relatively short-term asbestos exposures of ≤1–2 years or less, occurring up to 40 years in the past, have been associated with the development of mesotheliomas (an observation that emphasizes the importance of obtaining a complete environmental exposure history). Although the risk of mesothelioma is much less than that of lung cancer among asbestos-exposed workers, over 2000 cases were reported in the United States per year at the start of the twenty-first century.
Although ~50% of mesotheliomas metastasize, the tumor generally is locally invasive, and death usually results from local extension. Most patients present with effusions that may obscure the underlying pleural tumor. In contrast to the findings in effusion due to other causes, because of the restriction placed on the chest wall, no shift of mediastinal structures toward the opposite side of the chest will be seen. The major diagnostic problem is differentiation from peripherally spreading pulmonary adenocarcinoma or adenocarcinoma that has metastasized to pleura from an extrathoracic primary site. Although cytologic examination of pleural fluid may suggest the diagnosis, biopsy of pleural tissue, generally with video-assisted thoracic surgery, and special immunohistochemical staining usually are required. There is no effective therapy.
Since epidemiologic studies have shown that >80% of mesotheliomas may be associated with asbestos exposure, documented mesothelioma in a patient with occupational or environmental exposure to asbestos may be compensable.
Silicosis
In spite of being one of the oldest known occupational pulmonary hazards, free silica (SiO2), or crystalline quartz, is still a major cause of disease. The major occupational exposures include mining; stonecutting; employment in abrasive industries such as stone, clay, glass, and cement manufacturing; foundry work; packing of silica flour; and quarrying, particularly of granite. Most often, pulmonary fibrosis due to silica exposure (silicosis) occurs in a dose-response fashion after many years of exposure.
Workers heavily exposed through sandblasting in confined spaces, tunneling through rock with a high quartz content (15–25%), or the manufacture of abrasive soaps may develop acute silicosis with as little as 10 months of exposure. The clinical and pathologic features of acute silicosis are similar to those of pulmonary alveolar proteinosis . The chest radiograph may show profuse miliary infiltration or consolidation, and there is a characteristic HRCT pattern known as “crazy paving” (Fig. H-2). The disease may be quite severe and progressive despite the discontinuation of exposure. Whole-lung lavage may provide symptomatic relief and slow the progression.
Because silica is cytotoxic to alveolar macrophages, patients with silicosis are at greater risk of acquiring lung infections that involve these cells as a primary defense (Mycobacterium tuberculosis, atypical mycobacteria and fungi). Because of the increased risk of active tuberculosis, the recommended treatment of latent tuberculosis in these patients is longer. Another potential clinical complication of silicosis is autoimmune connective tissue disorders such as rheumatoid arthritis and scleroderma. In addition, there are sufficient epidemiologic data that the International Agency for Research on Cancer lists silica as a probable lung carcinogen.
Other, less hazardous silicates include fuller’s earth, kaolin, mica, diatomaceous earths, silica gel, soapstone, carbonate dusts, and cement dusts. The production of fibrosis in workers exposed to these agents is believed to be related either to the free silica content of these dusts or, for substances that contain no free silica, to the potentially large dust loads to which these workers may be exposed.
Other silicates, including talc dusts, may be contaminated with asbestos and/or free silica. Fibrosis and/or pleural or lung cancer have been associated with chronic exposure to commercial talc.
Coal Worker’s Pneumoconiosis (CWP)
Occupational exposure to coal dust can lead to CWP, which has enormous social, economic, and medical significance in every nation in which coal mining is an important industry. Simple radiographically identified CWP is seen in ~10% of all coal miners and in as many as 50% of anthracite miners with more than 20 years’ work on the coal face. The prevalence of disease is lower in workers in bituminous coal mines.
With prolonged exposure to coal dust (i.e., 15–20 years), small, rounded opacities similar to those of silicosis may develop. As in silicosis, the presence of these nodules (simple CWP) usually is not associated with pulmonary impairment. Much of the symptomatology associated with simple CWP appears to be due to the effects of coal dust on the development of chronic bronchitis and COPD . The effects of coal dust are additive to those of cigarette smoking.
Complicated CWP is manifested by the appearance on the chest radiograph of nodules ranging from 1 cm in diameter to the size of an entire lobe, generally confined to the upper half of the lungs. As in silicosis, this condition can progress to PMF that is accompanied by severe lung function deficits and associated with premature mortality. Despite improvements in technology to protect coal miners, cases of PMF still occur in the United States at a disturbing rate.
Caplan’s syndrome , first described in coal miners but subsequently found in patients with silicosis, includes seropositiverheumatoid arthritis with characteristic pneumoconiotic nodules. Silica has immunoadjuvant properties and is often present in anthracitic coal dust.
Chronic Beryllium Disease
Beryllium is a lightweight metal with tensile strength that has good electrical conductivity and is valuable in the control of nuclear reactions through its ability to quench neutrons. Although beryllium may produce an acute pneumonitis, it is far more commonly associated with a chronic granulomatous inflammatory disease that is similar to sarcoidosis . Unless one inquires specifically about occupational exposures to beryllium in the manufacture of alloys, ceramics, or high-technology electronics in a patient with sarcoidosis, one may miss entirely the etiologic relationship to the occupational exposure. What distinguishes chronic beryllium disease (CBD) from sarcoidosis is evidence of a specific cell-mediated immune response (i.e., delayed hypersensitivity) to beryllium.
The test that usually provides this evidence is the beryllium lymphocyte proliferation test (BeLPT). The BeLPT compares the in vitro proliferation of lymphocytes from blood or bronchoalveolar lavage in the presence of beryllium salts with that of unstimulated cells. Proliferation is usually measured by lymphocyte uptake of radiolabeled thymidine.
Chest imaging findings are similar to those of sarcoidosis (nodules along septal lines) except that hilar adenopathy is somewhat less common. As with sarcoidosis, pulmonary function test results may show restrictive and/or obstructive ventilatory deficits and decreased diffusing capacity. With early disease, both chest imaging studies and pulmonary function tests may be normal. Fiberoptic bronchoscopy with transbronchial lung biopsy usually is required to make the diagnosis of CBD. In a beryllium-sensitized individual, the presence of noncaseating granulomas or monocytic infiltration in lung tissue establishes the diagnosis. Accumulation of beryllium-specific CD4+ T cells occurs in the granulomatous inflammation seen on lung biopsy. CBD is one of the best studied examples of gene-environment interaction. Susceptibility to CBD is highly associated with human leukocyte antigen DP (HLA-DP) alleles that have a glutamic acid in position 69 of the B-chain.
Other metals, including aluminum and titanium dioxide, have been rarely associated with a sarcoid-like reaction in lung tissue. Exposure to dust containing tungsten carbide, also known as “hard metal,” may produce giant cell interstitial pneumonitis. Cobalt is a constituent of tungsten carbide and is the likely etiologic agent of both the interstitial pneumonitis and the occupational asthma that may occur. The most common exposures to tungsten carbide occur in tool and dye, saw blade, and drill bit manufacture. Diamond polishing may also involve exposure to cobalt dust. The same Glu69 polymorphism of the HLA-DP B-chain that confers increased risk of CBD also appears to increase the risk of cobalt-induced giant cell interstitial pneumonitis.
In patients with interstitial lung disease, one should always inquire about exposure to metal fumes and/or dusts. Especially when sarcoidosis appears to be the diagnosis, one should always consider possible CBD.
Other Inorganic Dusts
Most of the inorganic dusts discussed thus far are associated with the production of either dust macules or interstitial fibrotic changes in the lung. Other inorganic and organic dusts (see categories in Table H-1), along with some of the dusts previously discussed, are associated with chronic mucus hypersecretion (chronic bronchitis), with or without reduction of expiratory flow rates. Cigarette smoking is the major cause of these conditions, and any effort to attribute some component of the disease to occupational and environmental exposures must take cigarette smoking into account. Most studies suggest an additive effect of dust exposure and smoking. The pattern of the irritant dust effect is similar to that of cigarette smoking, suggesting that small airway inflammation may be the initial site of pathologic response in those cases and continued exposure may lead to chronic bronchitis and COPD.
Organic Dusts
Some of the specific diseases associated with organic dusts are discussed in detail in the chapters on asthma and hypersensitivity pneumonitis . Many of these diseases are named for the specific setting in which they are found, e.g., farmer’s lung, malt worker’s disease, and mushroom worker’s disease. Often the temporal relation of symptoms to exposure furnishes the best evidence for the diagnosis. Three occupational exposures are singled out for discussion here because they affect the largest proportions of workers.
Cotton Dust (Byssinosis)
Workers occupationally exposed to cotton dust (but also to flax, hemp, or jute dust) in the production of yarns for textiles and rope making are at risk for an asthma-like syndrome known as byssinosis. Exposure occurs throughout the manufacturing process but is most pronounced in the portions of the factory involved with the treatment of the cotton before spinning, i.e., blowing, mixing, and carding (straightening of fibers). The risk of byssinosis is associated with both cotton dust and endotoxin levels in the workplace environment.
Byssinosis is characterized clinically as occasional (early-stage) and then regular (late-stage) chest tightness toward the end of the first day of the workweek (“Monday chest tightness”). In epidemiologic studies, depending on the level of exposure via the carding room air, up to 80% of employees may show a significant drop in FEV1 over the course of a Monday shift.
Initially the symptoms do not recur on subsequent days of the week. However, in 10–25% of workers, the disease may be progressive, with chest tightness recurring or persisting throughout the workweek. After >10 years of exposure, workers with recurrent symptoms are more likely to have an obstructive pattern on pulmonary function testing. The highest grades of impairment generally are seen in smokers.
Reduction of dust exposure is of primary importance to the management of byssinosis. Dust levels can be controlled by the use of exhaust hoods, general increases in ventilation, and wetting procedures, but respiratory protective equipment appears to be required during certain operations to prevent workers from being exposed to levels of cotton dust that exceed the current OSHA-permissible exposure level. Regular surveillance of pulmonary function in cotton dust–exposed workers using spirometry before and after the workshift is required by OSHA. All workers with persistent symptoms or significantly reduced levels of pulmonary function should be moved to areas of lower risk of exposure.
Grain Dust
Worldwide, many farmers and workers in grain storage facilities are exposed to grain dust. The presentation of obstructive airway disease in grain dust–exposed workers is virtually identical to the characteristic findings in cigarette smokers, i.e., persistent cough, mucus hypersecretion, wheeze and dyspnea on exertion, and reduced FEV1 and FEV1/FVC (forced vital capacity) ratio.
Dust concentrations in grain elevators vary greatly but can be >10,000 µg/m3; approximately one-third of the particles, by weight, are in the respirable range. The effect of grain dust exposure is additive to that of cigarette smoking, with ~50% of workers who smoke having symptoms. Among nonsmoking grain elevator operators, approximately one-quarter have mucus hypersecretion, about five times the number that would be expected in unexposed nonsmokers. Smoking grain dust–exposed workers are more likely to have obstructive ventilatory deficits on pulmonary function testing. As in byssinosis, endotoxin may play a role in grain dust–induced chronic bronchitis and COPD.
Farmer’s Lung
This condition results from exposure to moldy hay containing spores of thermophilic actinomycetes that produce a hypersensitivity pneumonitis . A patient with acute farmer’s lung presents 4–8 h after exposure with fever, chills, malaise, cough, and dyspnea without wheezing. The history of exposure is obviously essential to distinguish this disease from influenza or pneumonia with similar symptoms. In the chronic form of the disease, the history of repeated attacks after similar exposure is important in differentiating this syndrome from other causes of patchy fibrosis (e.g., sarcoidosis).
A wide variety of other organic dusts are associated with the occurrence of hypersensitivity pneumonitis. For patients who present with hypersensitivity pneumonitis, specific and careful inquiry about occupations, hobbies, and other home environmental exposures is necessary to uncover the source of the etiologic agent.
Toxic Chemicals
Exposure to toxic chemicals affecting the lung generally involves gases and vapors. A common accident is one in which the victim is trapped in a confined space where the chemicals have accumulated to toxic levels. In addition to the specific toxic effects of the chemical, the victim often sustains considerable anoxia, which can play a dominant role in determining whether the individual survives.
Table H-2 lists a variety of toxic agents that can produce acute and sometimes life-threatening reactions in the lung. All these agents in sufficient concentrations have been demonstrated, at least in animal studies, to affect the lower airways and disrupt alveolar architecture, either acutely or as a result of chronic exposure. Some of these agents may be generated acutely in the environment (see below).
Table H-2 Selected Common Toxic Chemical Agents that Affect the Lung
| Agent(s) | Selected Exposures | Acute Effects from High or Accidental Exposure | Chronic Effects from Relatively Low Exposure |
| Acid anhydrides | Manufacture of resin esters, polyester resins, thermoactivated adhesives | Nasal irritation, cough | Asthma, chronic bronchitis, hypersensitivity pneumonitis |
| Acid fumes: H2SO4, HNO3 | Manufacture of fertilizers, chlorinated organic compounds, dyes, explosives, rubber products, metal etching, plastics | Mucous membrane irritation, followed by chemical pneumonitis 2–3 days later | Bronchitis and suggestion of mildly reduced pulmonary function in children with lifelong residential exposure to high levels |
| Acrolein and other aldehydes | By-product of burning plastics, woods, tobacco smoke | Mucous membrane irritant, decrease in lung function | Upper respiratory tract irritation |
| Ammonia | Refrigeration; petroleum refining; manufacture of fertilizers, explosives, plastics, and other chemicals | Same as for acid fumes, but bronchiectasis also has been reported | Upper respiratory tract irritation, chronic bronchitis |
| Cadmium fumes | Smelting, soldering, battery production | Mucous membrane irritant, acute respiratory distress syndrome (ARDS) | Chronic obstructive pulmonary disease (COPD) |
| Formaldehyde | Manufacture of resins, leathers, rubber, metals, and woods; laboratory workers, embalmers; emission from urethane foam insulation | Same as for acid fumes | Nasopharyngeal cancer |
| Halides and acid salts (Cl, Br, F) | Bleaching in pulp, paper, textile industry; manufacture of chemical compounds; synthetic rubber, plastics, disinfectant, rocket fuel, gasoline | Mucous membrane irritation, pulmonary edema; possible reduced FVC 1–2 yrs after exposure | Upper respiratory tract irritation, epistaxis, tracheobronchitis |
| Hydrogen sulfide | By-product of many industrial processes, oil, other petroleum processes and storage | Increase in respiratory rate followed by respiratory arrest, lactic acidosis, pulmonary edema, death | Conjunctival irritation, chronic bronchitis, recurrent pneumonitis |
| Isocyanates (TDI, HDI, MDI) | Production of polyurethane foams, plastics, adhesives, surface coatings | Mucous membrane irritation, dyspnea, cough, wheeze, pulmonary edema | Upper respiratory tract irritation, cough, asthma, hypersensitivity pneumonitis, reduced lung function |
| Nitrogen dioxide | Silage, metal etching, explosives, rocket fuels, welding, by-product of burning fossil fuels | Cough, dyspnea, pulmonary edema may be delayed 4–12 h; possible result from acute exposure: bronchiolitis obliterans in 2–6 wks | Emphysema in animals, ?chronic bronchitis, associated with reduced lung function in children with lifelong residential exposure |
| Ozone | Arc welding, flour bleaching, deodorizing, emissions from copying equipment, photochemical air pollutant | Mucous membrane irritant, pulmonary hemorrhage and edema, reduced pulmonary function transiently in children and adults, and increased hospitalization with exposure to summer haze | Excess cardiopulmonary mortality rates |
| Phosgene | Organic compound, metallurgy, volatilization of chlorine-containing compounds | Delayed onset of bronchiolitis and pulmonary edema | Chronic bronchitis |
| Sulfur dioxide | Manufacture of sulfuric acid, bleaches, coating of nonferrous metals, food processing, refrigerant, burning of fossil fuels, wood pulp industry | Mucous membrane irritant, epistaxis, bronchospasm (especially in people with asthma) | Chronic bronchitis |
Firefighters and fire victims are at risk of smoke inhalation, an important cause of acute cardiorespiratory failure. Smoke inhalation kills more fire victims than does thermal injury. Carbon monoxide poisoning with resulting significant hypoxemia can be life-threatening . Synthetic materials (plastic, polyurethanes), when burned, may release a variety of other toxic agents (such as cyanide and hydrochloric acid), and this must be considered in evaluating smoke inhalation victims. Exposed victims may have some degree of lower respiratory tract inflammation and/or pulmonary edema.
Exposure to certain highly reactive, low-molecular-weight agents used in the manufacture of synthetic polymers, paints, and coatings (diisocyanates in polyurethanes, aromatic amines and acid anhydrides in epoxies) are associated with a high risk of occupational asthma. Although this occupational asthma manifests clinically as if sensitization has occurred, an IgE antibody–mediated mechanism is not necessarily involved. Hypersensitivity pneumonitis–like reactions also have been described in diisocyanate and acid anhydride–exposed workers.
Fluoropolymers such as Teflon, which at normal temperatures produce no reaction, become volatilized upon heating. The inhaled agents cause a characteristic syndrome of fever, chills, malaise, and occasionally mild wheezing, leading to the diagnosis of polymer fume fever. A similar self-limited, influenza-like syndrome— metal fume fever—results from acute exposure to fumes or smoke containing zinc oxide. The syndrome may begin several hours after work and resolves within 24 h, only to return on repeated exposure. Welding of galvanized steel is the most common exposure leading to metal fume fever.
Two other agents have been recently associated with potentially severe interstitial lung disease. Occupational exposure to nylon flock has been shown to induce a lymphocytic bronchiolitis, and workers exposed to diacetyl used to provide “butter” flavor in the manufacture of microwave popcorn and other foods have developed bronchiolitis obliterans .
World Trade Center Disaster
consequence of the attack on the World Trade Center (WTC) on September 11, 2001, was relatively heavy exposure of a large number of firefighters and other rescue workers to the dust generated by the collapse of the buildings. Environmental monitoring and chemical characterization of WTC dust has revealed a wide variety of potentially toxic constituents, although much of the dust was pulverized cement. Possibly because of the high alkalinity of WTC dust, significant cough, wheeze, and phlegm production occurred among firefighters and cleanup crews. New cough and wheeze syndromes also occurred among local residents. Initial longitudinal follow-up of New York firefighters suggests that heavier exposure to WTC dust is associated with accelerated decline of lung function. Ongoing follow-up will provide data on whether massive exposure to this irritant dust has led to the development of chronic respiratory disease.
Occupational Respiratory Carcinogens
Exposures at work have been estimated to contribute to 10% of all lung cancer cases. In addition to asbestos, other agents either proven or suspected to be respiratory carcinogens include acrylonitrile, arsenic compounds, beryllium, bis(chloromethyl) ether, chromium (hexavalent), formaldehyde (nasal), isopropanol (nasal sinuses), mustard gas, nickel carbonyl (nickel smelting), polyaromatic hydrocarbons (coke oven emissions and diesel exhaust), secondhand tobacco smoke, silica (both mining and processing), talc (possible asbestos contamination in both mining and milling), vinyl chloride (sarcomas), wood (nasal cancer only), and uranium. Workers at risk of radiation-related lung cancer include not only those involved in mining or processing uranium but also those exposed in underground mining operations of other ores where radon daughters may be emitted from rock formations.
Assessment of Disability
Patients who have lung disease may not be able to continue to work in their usual jobs because of respiratory symptoms. Disability is the term used to describe the decreased ability to work due to the effects of a medical condition. Physicians are generally able to assess physiologic dysfunction, or impairment, but the rating of disability for compensation of loss of income also involves nonmedical factors such as the education and employability of the individual. The disability rating scheme differs with the compensation-granting agency. For example, the U.S. Social Security Administration requires that an individual be unable to do any work (i.e., total disability) before he or she will receive income replacement payments. Many state workers’ compensation systems allow for payments for partial disability. In the Social Security scheme no determination of cause is done, whereas work-relatedness must be established in workers’ compensation systems.
For respiratory impairment rating, resting pulmonary function tests (spirometry and diffusing capacity) are used as the initial assessment tool, with cardiopulmonary exercise testing (to assess maximal oxygen consumption) used if the results of the resting tests do not correlate with the patient’s symptoms. Methacholine challenge (to assess airway reactivity) can also be useful in patients with asthma who have normal spirometry when evaluated. Some compensation agencies (e.g., Social Security) have proscribed disability classification schemes based on pulmonary function test results. When no specific scheme is proscribed, the Guidelines of the American Medical Association should be used.
Evaluating relation to work exposure requires a detailed work history, as previously discussed in this chapter. Occasionally, as with some cases of suspected occupational asthma, challenge to the putative agent in the work environment with repeated pulmonary function measures may be required.
General Environmental Exposures
Outdoor Air Pollution
In 1971, the U.S. government established national air quality standards for several pollutants believed to be responsible for excess cardiorespiratory diseases. Primary standards regulated by the U.S. Environmental Protection Agency (EPA) designed to protect the public health with an adequate margin of safety exist for sulfur dioxide, particulates matter, nitrogen dioxide, ozone, lead, and carbon monoxide. Standards for each of these pollutants are updated regularly through an extensive review process conducted by the EPA.
Pollutants are generated from both stationary sources (power plants and industrial complexes) and mobile sources (automobiles), and none of the regulated pollutants occurs in isolation. Furthermore, pollutants may be changed by chemical reactions after being emitted. For example, sulfur dioxide and particulate matter emissions from a coal-fired power plant may react in air to produce acid sulfates and aerosols, which can be transported long distances in the atmosphere. Oxidizing substances such as oxides of nitrogen and volatile organic compounds from automobile exhaust may react with sunlight to produce ozone. Although originally thought to be confined to Los Angeles, photochemically derived pollution (“smog”) is now known to be a problem throughout the United States and in many other countries. Both acute and chronic effects of these exposures have been documented in large population studies.
The symptoms and diseases associated with air pollution are the same as conditions commonly associated with cigarette smoking. In addition, decreased growth of lung function and asthma have been associated with chronic exposure to only modestly elevated levels of traffic-related gases and respirable particles. Multiple population-based time-series studies within cities have demonstrated excess health care utilization for asthma and other cardiopulmonary conditions and mortality rates. Cohort studies comparing cities that have relatively high levels of particulate exposures with less polluted communities suggest excess morbidity and mortality rates from cardiopulmonary conditions in long-term residents of the former. The strong epidemiologic evidence that fine particulate matter is a risk factor for cardiovascular morbidity and mortality has prompted toxicologic investigations into the underlying mechanisms. The inhalation of fine particles from combustion sources probably generates oxidative stress followed by local injury and inflammation in the lungs that in turn lead to autonomic and systemic inflammatory responses that can induce endothelial dysfunction and/or injury. Recent research findings on the health effects of air pollutants have led to stricter U.S. ambient air quality standards for ozone, oxides of nitrogen, and particulate matter as well as greater emphasis on publicizing pollution alerts to encourage individuals with significant cardiopulmonary impairment to stay indoors during high-pollution episodes.
Indoor Exposures
Secondhand tobacco smoke , radon gas, wood smoke, and other biologic agents generated indoors must be considered. Several studies have shown that the respirable particulate load in any household is directly proportional to the number of cigarette smokers living in that home. Increases in prevalence of respiratory illnesses, especially asthma, and reduced levels of pulmonary function measured with simple spirometry have been found in the children of smoking parents in a number of studies. Recent meta-analyses for lung cancer and cardiopulmonary diseases, combining data from multiple secondhand tobacco smoke epidemiologic studies, suggest an ~25% increase in relative risk for each condition, even after adjustment for major potential confounders.
Exposure to radon gas in homes is a risk factor for lung cancer. The main radon product (radon 222) is a gas that results from the decay series of uranium 238, with the immediate precursor being radium 226. The amount of radium in earth materials determines how much radon gas will be emitted. Outdoors, the concentrations are trivial. Indoors, levels are dependent on the sources, the ventilation rate of the space, and the size of the space into which the gas is emitted. Levels associated with excess lung cancer risk may be present in as many as 10% of the houses in the United States. When smokers reside in the home, the problem is potentially greater, since the molecular size of radon particles allows them to attach readily to smoke particles that are inhaled. Fortunately, technology is available for assessing and reducing the level of exposure.
Other indoor exposures of concern are bioaerosols that contain antigenic material (fungi, cockroaches, dust mites, and pet danders) associated with an increased risk of atopy and asthma. Indoor chemical agents include strong cleaning agents (bleach, ammonia), formaldehyde, perfumes, pesticides, and oxides of nitrogen from gas appliances. Nonspecific responses associated with “tight-building syndrome,” perhaps better termed “building-associated illness,” in which no particular agent has been implicated, have included a wide variety of complaints, among them respiratory symptoms that are relieved only by avoiding exposure in the building in question. The degree to which “smells” and other sensory stimuli are involved in the triggering of potentially incapacitating psychological or physical responses has yet to be determined, and the long-term consequences of such environmental exposures are unknown.
Portal of Entry
The lung is a primary point of entry into the body for a number of toxic agents that affect other organ systems. For example, the lung is a route of entry for benzene (bone marrow), carbon disulfide (cardiovascular and nervous systems), cadmium (kidney), and metallic mercury (kidney, central nervous system). Thus, in any disease state of obscure origin, it is important to consider the possibility of inhaled environmental agents. Such consideration can sometimes furnish the clue needed to identify a specific external cause for a disorder that might otherwise be labeled “idiopathic.”
Global Considerations
Indoor exposure to biomass smoke (wood, dung, crop residues, charcoal) is estimated to be responsible for ~3% of worldwide disability-adjusted life-years (DALYs) lost, due to acute lower respiratory infections in children and COPD and lung cancer in women. This burden of disease places indoor exposure to biomass smoke as the second leading environmental hazard for poor health, just behind unsafe water, sanitation, and hygiene, and is 3.5 times larger than the burden attributed to outdoor air pollution.
More than one-half of the world’s population uses biomass fuel for cooking, heating, or baking. This occurs predominantly in the rural areas of developing countries. Because many families burn biomass fuels in open stoves, which are highly inefficient, and inside homes with poor ventilation, women and young children are exposed on a daily basis to high levels of smoke. In these homes, 24-h mean levels of fine particulate matter, a component of biomass smoke, have been reported to be 2–30 times higher than the National Ambient Air Quality Standards set by the U.S. EPA.
Epidemiologic studies have consistently shown associations between exposure to biomass smoke and both chronic bronchitis and COPD, with odds ratios ranging between 3 and 10 and increasing with longer exposures. In addition to the common occupational exposure to biomass smoke of women in developing countries, men from such countries may be occupationally exposed. Because of increased migration to the United States from developing countries, clinicians need to be aware of the chronic respiratory effects of exposure to biomass smoke, which can include interstitial lung disease (Fig. H-4). Evidence is beginning to emerge that improved stoves with chimneys can reduce biomass smoke–induced respiratory illness in both children and women.
 _U.S. Dollar
_U.S. Dollar _Nepali Rupees
_Nepali Rupees